

INTRODUCTION
Tetracycline antibiotics inhibit protein synthesis and are broad-spectrum agents that are useful in a wide range of gram-positive and gram-negative bacteria, mycoplasmas, chlamydia, protozoans, rickettsia, and other microbes.1 They also inhibit proinflammatory cytokines and neutrophil chemotaxis and reduce sebum free fatty acids and bacterial lipases, thus also giving them anti-inflammatory and immunosuppressive properties. Therefore, they are also useful in managing conditions such as acne vulgaris, rosacea, and rheumatologic and immunobullous disorders.2–4
Commonly used semisynthetic tetracyclines include minocycline (7-dimethylamino-6-demethyl-6-deoxytetracycline) and doxycycline (6-deoxy-5-hydroxytetracycline); doxycycline is available in two forms: hyclate, which is water soluble, or monohydrate, which is only slightly water soluble.1 Minocycline and doxycycline both have long elimination half-lives, which reduces the dosing needed to maintain desired serum concentrations. They are lipid soluble and penetrate well into tissues, body fluids, and even sebum and are excreted in perspiration.1 These drugs are expelled in the urine.1
Oxidation of tetracyclines leads to the formation of complexes that typically include iron, melanin, hemosiderin, ferritin, or others, causing it to turn from its typical crystalline yellow material to black.4,5 They—especially minocycline but largely excluding doxycycline—have been known to cause hyperpigmentation throughout the body, including the thyroid, bone, skin, gums and oral mucosa, teeth, nails, and sclera, among other locations, including the bone of the orbital rim found incidentally on lacrimal gland biopsy.2,4–9 Of note, only 18 patients have been reported in the literature to have doxycycline-associated skin hyperpigmentation; on the other hand, more than 20% of those on minocycline for longer than 4 years develop pigmentation of the oral cavity bones, making it the most frequently affected site.2,6
The incidence of minocycline-induced hyperpigmentation reported varies depending on the disease for which it is being used; although the overall incidence is low, it is notably higher in immunobullous disorders such as pemphigus or pemphigoid.4 For example, in those with acne, the incidence of cutaneous hyperpigmentation is approximately 2.4%-14.8%; it was 2.75% in those with rheumatoid arthritis in one series, but 55.6% in pemphigus and pemphigoid.4,7,10–12
Cutaneous hyperpigmentation may morphologically appear as type I: black or blue-gray pigmented macules localized to areas of scarring, prior injury, or inflammation; type II: circumscribed or diffuse blue-gray pigmentation of normal skin, most often the shins, ankles, or arms; or type III: diffuse muddy brown hyperpigmentation that is accentuated in sun-exposed areas.2,5,13 Histological analyses from skin biopsy specimens have found pigment-laden macrophages in the dermis and adipocytes.4 Pigmentation generally occurs with cumulative doses of more than 70-100 g, although it can be seen at any dose or duration in the oral mucosa or in type I skin pigmentation.2 Oral mucosa and cutaneous type I pigmentation typically gradually reverses after discontinuation, fading over the course of up to several years; however, it is often permanent at other sites.2,5 Although this hyperpigmentation is not detrimental, aside from cosmesis, stopping the drug and avoiding sun exposure is generally recommended.
Ocular involvement is uncommon and is usually only seen after high-dose, long-duration use; most reports of eye-related pigmentation involve the sclera.2 Here, we present three cases of nonscleral ocular pigmentation associated with tetracycline derivatives.
CASE REPORTS
Case 1
This 60-year-old White male had 20/20 acuity in both eyes and had no ocular history. He had benign prostatic hypertrophy, osteoarthritis, hypertension, and widespread acne. Medications included tamsulosin, meloxicam, and amlodipine. He had also been taking minocycline 100 mg per day for almost 30 years. He developed bluish-gray lateral bulbar scleral hyperpigmentation with an otherwise unremarkable eye examination, along with type II cutaneous hyperpigmentation that was most visible on and anterior to his tragus (Figure 1). The sclerae have remained stable whereas the cutaneous hyperpigmentation has increased after 2 additional years of monitoring while continuing on minocycline.
_minocycline-induced_type_ii_hyperpigmentation_of_bilateral_facial_skin_on_.png)
Case 2
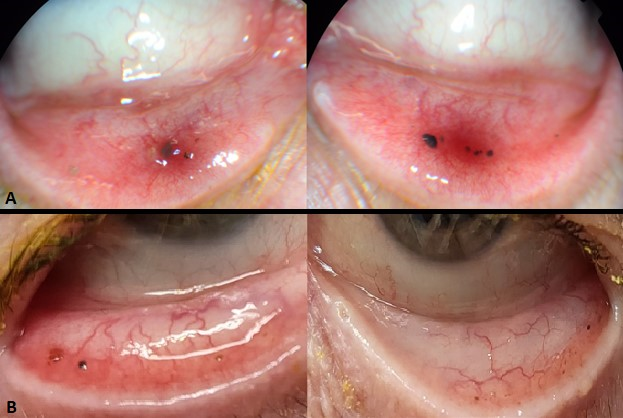
This 62-year-old White male had hypertension, hypercholesterolemia, and gout; his medications included amlodipine, hydrochlorothiazide/lisinopril, metoprolol tartrate, simvastatin, and colchicine. He was also treated with doxycycline 100 mg twice per day for approximately 4 years for facial rosacea with phymatous, ocular/eyelid, and erythmatotelangiectatic features. Then, at age 66, his other medications remained unchanged but doxycycline was changed to minocycline 100 mg twice per day. Approximately 7 months later, he was noted to have multiple small dark spots on his bilateral lower legs. Approximately 2 months after that, he had a normal eye examination, including 20/20 best-corrected acuity in both eyes. However, at his next eye examination (approximately 28 months after starting minocycline), he was found to have several small gray and black deposits, some that were in clusters, encapsulated in small surrounding clear cysts in the palpebral conjunctiva and inferior fornix (Figure 2) with otherwise stable and unremarkable eye examination findings. By that time, the lower-extremity hyperpigmentation progressed to become dense, spotted dark bluish-gray macules coalescing into large patches on the bilateral dorsal feet and bilateral lower extremities (Figure 3), which dermatology attributed to type II minocycline-induced hyperpigmentation. Discontinuation of minocycline was recommended, but the patient felt the minocycline was helping control his facial rosacea and was only minimally concerned cosmetically by the hyperpigmentation; thus, he elected to continue minocycline. Conjunctival and bilateral-lower extremity findings were similar on examination another 29 months thereafter.

_bilateral_lower_extremiti.png)
Case 3
This 63-year-old White male had a history of chronic lateral epicondylitis, chronic left shoulder pain from a bone spur, prostate cancer status post radical prostatectomy, hypertension, burning mouth syndrome, and an incisional hernia from gallbladder surgery. He was taking gabapentin, hydrocodone/acetaminophen, phenazopyridine, simvastatin, tamsulosin, and zolpidem. He had also been taking doxycycline 100 mg per day for 8 years for cystic acne on his scalp and was noted to have bilateral lower palpebral conjunctival brown pigmented concretion-like deposits (Figure 2); at that time, his cumulative dose of doxycycline was 292 g. He had had an unremarkable eye examination 20 months prior with 20/20 best-corrected acuity in both eyes. He was not found to have hyperpigmentation elsewhere at that time or since, including an examination of his legs and alveolar mucosa. He has been followed for more than 8 additional years and continues to demonstrate conjunctival pigmentation without any other areas of hyperpigmentation.
Case 4
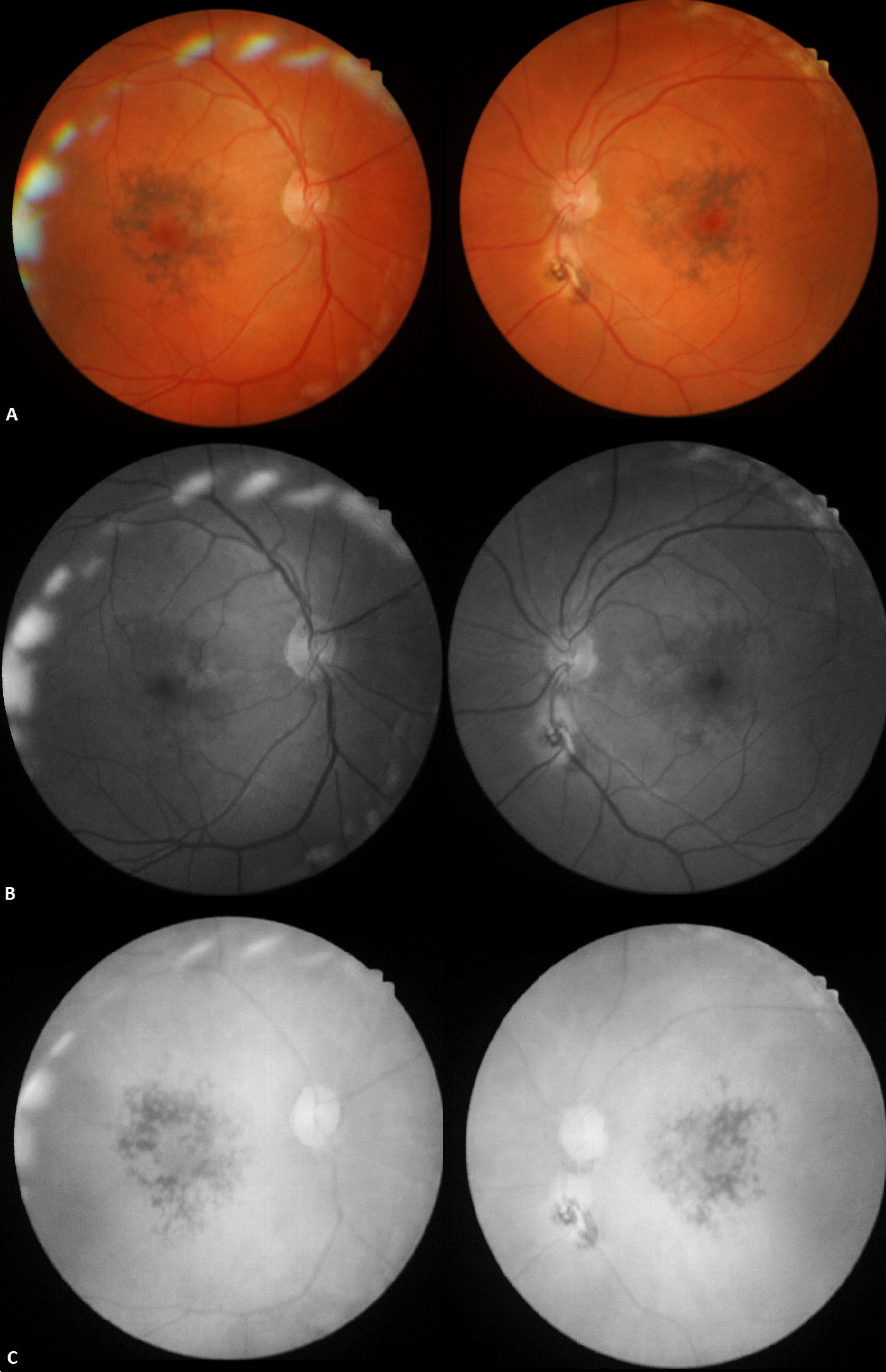
This 53-year-old White male had mild cerebral palsy with cognitive disability and lived in a group home. He was pseudophakic in both eyes and had undergone a laser capsulotomy in the left eye. His medical history additionally included gastroesophageal reflux disease, urinary incontinence, depression, hypercholesterolemia, vitamin D deficiency, asthma, seasonal allergies, and hypothyroidism. Medications included omeprazole, oxybutynin, paroxetine, simvastatin, vitamin D, montelukast, budesonide, albuterol, fexofenadine, and levothyroxine. He also had been taking minocycline 100 mg per day for more than 10 years for acne vulgaris. He reported no visual symptoms, but best-corrected acuity was reduced to 20/30 in each eye. He was found to have conjunctival hyperpigmentation along with striking pigmentary changes in the macula of both eyes (Figure 4). He also had an unrelated chorioretinal scar inferior to the left optic disc, but otherwise, his eye examination was unremarkable. The areas of macular hyperpigmentation were mildly hypointense versus background, or the contrast between the hyperpigmentation and background was diminished on green (red-free filter). It was notably darker versus background, or it showed greater contrast between the pigmentation and background on red (green-free) filter. These indicate that the hyperpigmentation localized below the level of the retinal pigmented epithelium. Clinical examination, imaging as described, and coexisting conjunctival hyperpigmentation all implicated minocycline-associated macular hyperpigmentation. Because of the macular changes, minocycline was discontinued. The macular findings were stable approximately 2 years later.
_color.png)
None of the other medications taken by any of these patients have been known to cause cutaneous, scleral, macular, or conjunctival hyperpigmentation.
DISCUSSION
Sclera
The sclera has been the most-reported area of ocular hyperpigmentation associated with tetracycline derivatives. Scleral involvement is usually either a diffuse blue discoloration or a blue-gray lateral limbal band, although more consolidated spots have been described.5,8,14–19 When the sclera is involved, nails are almost universally affected as well, and various other sites may be involved.2,8 These patients typically have had more than 2 years of use, and most have exhibited cutaneous hyperpigmentation, typically type III, suggesting that scleral involvement occurs with more severe pigmentary changes.2,8,18
Differentials for scleral or conjunctival pigmentary changes include exposure to heavy metals (such as gold, mercury, copper, or iron), argyrosis (silver deposition), drugs (such as epinephrine, phenothiazines, or antimalarials), scleromalacia perforans, or melanocytic tumors.8,20 When there is concern for heavy metal or silver exposure, case history is vital but serum levels can also be evaluated; the discoloration from metal particle deposition can also be biopsied for confirmation. Case history is also important to rule out other medications known to potentially cause ocular hyperpigmentation. Scleromalacia perforans gives a grayish-blue appearance caused by increased visibility of the underlying choroid but, unlike hyperpigmentation, is associated with scleral thinning. Melanocytic tumors are more likely to be solitary, whereas hyperpigmentation in this context is multifocal or diffuse; they, too, can be biopsied for differentiation.
Conjunctiva
Prior cases of minocycline-associated conjunctival hyperpigmentation, typically seen within inclusion cysts of the palpebral conjunctiva, have been sparse, and other areas of hyperpigmentation in these cases have been variable; notably, they may occur with or without skin involvement. We are aware of only 14 patients on long-term tetracycline and/or its derivatives who have been reported to develop palpebral conjunctival hyperpigmentation, but to our knowledge, no tetracycline-naive patients on doxycycline alone have previously been reported to develop conjunctival hyperpigmentation (Table 1).20–23
In 1981, Brothers and Hidayat’s patient, who had taken tetracycline then minocycline, presented with dark spots in the medial and lateral upper tarsi and laterally in the bilateral lower tarsi. They were described as granular, crystalline-like deposits of various sizes that were dark brown to black, often in clusters of up to 2 mm, and surrounded by small cysts and/or gray-white soft spots.20 The patient did not have skin or nailbed hyperpigmentation. The conjunctival deposits histologically were concretions in conjunctival cysts, showing laminated brownish concretions that autofluoresced under ultraviolet light and stained positively for calcium; they proposed that tetracycline had formed extracellular chelation complexes with calcium, causing the pigmentation.20
In 1983, Messmer et al. presented a case, also on tetracycline then minocycline, of bilateral lateral lower palpebral conjunctival intracystic epithelial inclusions that were both pigmented and unpigmented and ranged from <1 to 2 mm.21 The most similar-appearing clinical differential diagnosis was foreign bodies, consistent with our experience. The contents of the cysts were moderately electron-dense amorphous material and epithelial cells that were degenerating by electron microscopy. Histochemically, the pigment was thought to represent a product of tetracycline oxidation. By light microscopy, there was eosinophilic globular material or laminated eosinophilic to brownish concretions that demonstrated the yellowish-green autofluorescence characteristic of tetracyclines.21 As an important clinical point, using the cobalt blue filter at the slit lamp, these pigmented spots in the conjunctiva are known to autofluoresce.24,25
Subsequently, 12 patients have been reported with similar tetracycline-associated palpebral conjunctival pigmentation. Of these, one also had pigmentation of the caruncle; five had scleral involvement, and among those with scleral involvement, one had hyperpigmentation of the skin (type II), nails, and teeth and another had diffuse pigmentation of the skin; three had macular retinal pigmented epithelium clumping.8,18,19,24–30 There has also been one additional report of dark green granular deposits on the temporal bulbar conjunctiva associated with tetracycline use.31
Macula
Bradfield et al. first reported minocycline-associated retinal hyperpigmentation in 2003 in a photo essay. Their patient, a 70-year-old White woman, had taken minocycline for 5 years (dose not noted) for rheumatoid arthritis and showed conjunctival pigment along with discrete retinal pigment epithelium clumps in both maculae, which blocked background fluorescence on fluorescein angiography (Table 2).19
Next, reported by Wilson et al. in 2015, a man taking 100 mg minocycline twice per day for more than 30 years showed similar conjunctival and macular findings, along with scleral and nailbed hyperpigmentation; their work demonstrated nodular retinal pigmented epithelium deposits between Bruch’s membrane and the retinal pigmented epithelium on spectral domain optical coherence tomography, and no abnormal fluorescence pattern on fluorescein angiography.29 This patient had no visual complaints and normal visual acuity.
Then, Jung et al. in 2016 reported a case of diffuse slate-gray hyperpigmentation of the arms and face (type II), conjunctiva, and sclera and confluent black pigmented deposits in the fovea between the retinal pigmented epithelium and Bruch’s membrane, attributed to minocycline-induced hyperpigmentation.27 This patient had taken minocycline for 15 years, and the only visual symptom related to this was mild metamorphopsia. Green wavelength fundus autofluorescence indicated minimal hypo-autofluorescence in both eyes with some speckled hyper-autofluorescence in one eye. Jung proposed that, because lipofuscin content tends to increase as retinal pigmented epithelium cells become more diseased, and fused melanolipofuscin granule content likely rises with chronic medication use, the lipofuscin accounted for the speckled hyper-autofluorescence pattern that was observed. Lipofuscin hyperautofluoresces at shorter wavelengths (i.e., with green wavelength autofluorescence); melanin, on the other hand, may be more autofluorescent at longer wavelengths (near infrared) so does not demonstrate any notable fundus autofluorescence pattern on the typical green wavelength fundus autofluorescence imaging platform.27 Swept-source optical coherence tomography findings echoed that of Bradfield, indicating confluent pigment epithelial detachments, similar to drusen in appearance, between Bruch’s membrane and the retinal pigmented epithelium. The outer retina was otherwise undisturbed. Because there is greater melanin content in the macular region, specifically concentrated in the retinal pigmented epithelium cells of the fovea, Jung suggested that this hyperpigmentation is from minocycline oxidation forming pigmented complexes with the melanin and is thus most predominant in the macula. Optical coherence tomography-angiography was normal in the retina, but there was notable blocking of the choriocapillaris due to the increased pigment. This patient’s macular hyperpigmentation was persistent 1 year after discontinuation of minocycline.
Our patient in Case 4 had both conjunctival and macular hyperpigmentation. Photos were similar to those offered by Bradfield, Jung, and Wilson; red and green filter photos indicate that the hyperpigmentation is below the level of the retinal pigmented epithelium, consistent with the previously noted reports of this hyperpigmentation being localized between Bruch’s membrane and the retinal pigmented epithelium. This is the fourth reported case of minocycline-associated macular pigmentation.
Other drugs have been known to cause pigmentary changes in the macula. For example, phenothiazines may cause granular stippling of macular pigment with early toxicity but later leads to atrophy of and surrounding the retinal pigmented epithelium.32 The antimalarial drug chloroquine and its derivatives are well known to cause pigmentary maculopathy, although this primarily involves hypopigmentation due to retinal pigmented epithelial atrophy in a classic bulls eye pattern.32 Pentosan polysulfate sodium has more recently been reported to cause a pigmentary maculopathy after 15-20 years of long-term use. This presents with patchy parafoveal atrophic spots and pigmented deposits within the retinal pigmented epithelium, along with foci of vitelliform material, which demonstrate speckled hyperautofluorescence.32 Macular hyperpigmentation or similar clinical presentations may also be seen in the context of prior trauma or related to various pattern retinal dystrophies or various degenerations. In patients with tetracycline-associated macular hyperpigmentation, positive history for use of the medication and hyperpigmentation elsewhere (such as the conjunctiva, sclera, nailbed, or skin) are expected.
CONCLUSION
To our knowledge, after review of available literature, there have previously been 15 reported cases of minocycline-induced conjunctival hyperpigmentation. Here, we add three cases, including the first reported case of tetracycline-naive doxycycline-associated conjunctival pigmentation and one that is the fourth reported case of minocycline-associated macular hyperpigmentation. Conjunctival, and especially retinal, changes have been thought to be late manifestations of minocycline-associated hyperpigmentation.18 Interestingly, however, our Case 3 patient who had doxycycline-associated conjunctival pigmentation had no other visible areas of hyperpigmentation, suggesting that perhaps it may be an earlier manifestation of doxycycline hyperpigmentation.
Because tetracycline and its derivatives are used so frequently across medical disciplines for many conditions, hyperpigmentation should be routinely screened for and discussed with patients.
Take Home Points
-
Tetracyclines may cause hyperpigmentation throughout the body.
-
Ocular hyperpigmentation may involve the sclera, conjunctiva or macula.
-
Hyperpigmentation due to tetracyclines should be routinely screened for and discussed with patients.
Patient consent
No identifiable health information is included in these case reports.
Institutional review board approval was not required per institutional determination. The institutional privacy officer confirmed this manuscript complies with institutional privacy policy.
ACKNOWLEDGMENTS
None.
DISCLOSURES AND CONFLICT OF INTEREST
The authors declare no conflicts of interest.
AUTHOR CONTRIBUTIONS
Weidmayer: Conceptualization, data curation, writing-original draft.
Borgman: Data curation, writing-review and editing.