
INTRODUCTION
To overcome diagnostic challenges that are associated with symptoms of seeing more than one image, an understanding of terms and their origins are critical. Here, we provide a background to the various visual symptoms that presented in our patient.
Diplopia is a relatively common complaint heard among health care professionals and can be understood by the Greek root words of diplo, meaning “double,” and opia, meaning “vision.” The majority of the time, diplopia occurs bilaterally rather than monocularly.1 Causes of monocular diplopia include refractive error, compression of the globe by the eyelid, tear film abnormalities, corneal opacities, corneal dystrophies or degenerations, refractive surgery complications, cataracts, lenticular malposition, lenticular misshape, iris deformities, vitreous foreign bodies, maculopathies, or central nervous system abnormalities.2,3 The causes may be grouped into three categories: light diffraction, metamorphopsia, and cerebral polyopia.2 Light diffraction occurs in cases of ocular disease in which images from a single object are split and fall on different areas of the retina. Diffraction-induced monocular diplopia occurs because of the lens more often than the cornea whereas vitreous causes are rare.4 Metamorphopsia entails retinal pathology such as epiretinal membranes or macular edema.2,3 Cerebral polyopia arises from either the occipital lobe or along the central visual pathway and may occur in cases such as migraines, occipital lobe seizures, tumors, or occipital lobe infarcts.5,6 The most common cause of monocular diplopia is refractive error,7 and refractive surgery is also a common cause.8
The term palinopsia was coined in 1951 by Critchley and is derived from the Greek word palin, meaning “again,” and opsia, meaning “seeing,” and was later described by Bender as “the persistence or recurrence of visual images after the stimulus has been removed.”9,10 It is also commonly referred to as visual preservation.9 Previously, palinopsia was subdivided into “immediate,” if it occurs within seconds of a stimulus, or “delayed,” if it occurs seconds after a stimulus.11 Now, palinopsia is considered to have eight distinct symptomology-derived subtypes, including forced image preservation, scene preservation, categorical corporation, illusory visual spread, prolonged indistinct afterimage, light streaking, visual trailing, and variant image preservation.12 Causes of palinopsia include space-occupying post-geniculate cortical lesions, cerebrovascular accidents, arteriovenous malformations, aneurysms, cortical deafferentation hyperexcitability, seizures, neurosurgical procedures, hyperglycemia, transient ischemic attacks, cortical pathology, demyelination, illicit drugs, prescription drugs, neurotransmitter and neurotransmitter receptor alterations, migraines, head trauma, and psychiatric conditions.12 The repeated images may occur immediately after a visual stimulus or may occur even days after the original stimulus.13 Although palinopsia is commonly referred to as a visual hallucination, it is not technically a hallucination in the strictest sense of the word, as it is not a perception of an external stimulus without a source in the external world14 as it really is an enhancement or a creation of an afterimage.14 In the literature, the terminology and definitions surrounding palinopsia are contested, but the principle of a recurring visual image after removal of the original stimulus remains.
Photopsia is a Greek word derived from photizein, meaning “to give light,” and opsia, meaning “to see,” and is described as a sudden onset, transient flash of light occurring without light entering the eye. When unilateral, the potential causes include posterior vitreous detachment, phosphenes from eye rubbing or eye movement, age-related macular degeneration, central serous chorioretinopathy, retinal and choroidal inflammatory conditions, retinal or choroidal neoplasms, retinal artery occlusion, or unilateral disc swelling.15 When bilateral, the potential causes include papilledema, retinal or choroidal neoplasms, Charles Bonnet syndrome, migraine with aura, aura without migraine, epilepsy, cerebrovascular accident, inflammatory or infectious encephalopathies, cortical neoplasms, illicit drugs, or prescription drugs.15 Photopsia primarily occurs owing to a posterior vitreous detachment, retinal tear or detachment, migraines with an aura, or an aura without a migraine.16
CASE REPORT
A 33-year-old woman presented with a complaint of monocular diplopia of both eyes individually along with palinopsia and photopsia of both eyes. The monocular diplopia of each eye individually was both vertical and horizontal in nature and seemed to fluctuate in severity. The palinopsia only occurred with object movement, and the most recognizable visual stimulus eliciting palinopsia was when she moved her hand in front of her and subsequently visualized three or four trailing hand images (Figure 1). The photopsia occurred in each eye individually in random locations and only at night.

Her past ocular history included LASIK performed in Mexico 11 years prior with no complications. Her past medication history was significant for thrombocytopenia, B12 deficiency, otalgia of both ears, preeclampsia, anemia, history of COVID-19, depression with anxiety, facial pain, fatigue, intermittent lightheadedness, paresthesia, and migraines. She was taking no ocular mediations. She had begun taking topiramate 50 mg by mouth twice daily for migraines 5 months before this eye examination, and her visual disturbance onset was 2 months after first taking topiramate. Her other systemic medications included cyanocobalamin 1000 μg by mouth daily for vitamin B12 deficiency and ferrous sulfate 325 mg by mouth every morning for anemia. Magnetic resonance imaging of the brain with and without contrast was performed the week before beginning topiramate and showed only minimal ethmoid and maxillary sinus mucosal thickening with a left maxillary sinus mucous retention cyst. The mastoid air cells were clear. The orbital structures appeared normal.
Her uncorrected vision was 20/20 in each eye individually. There was no afferent pupillary defect in either eye. Applanation tonometry was 14 mm Hg pressure in each eye. Extraocular movements were full. Cover testing revealed two exophoria at distance and six exophoria at near with no tropia. Slit lamp examination demonstrated a pinpoint spot of posterior subcapsular cataract in the lens of the left eye only but was otherwise unremarkable. The posterior segment examination was unremarkable sans a slightly tilted optic disc of the left eye.
The manifest refraction yielded 20/15 vision in the right eye and 20/20 vision in the left eye, and the results are detailed below. The manifest refraction, right eye: +0.25 -0.50 × 022 and left eye: +0.25 -0.25 × 175, did not relieve the monocular diplopia or the other visual disturbances. The patient was alert and oriented with a calm demeanor.
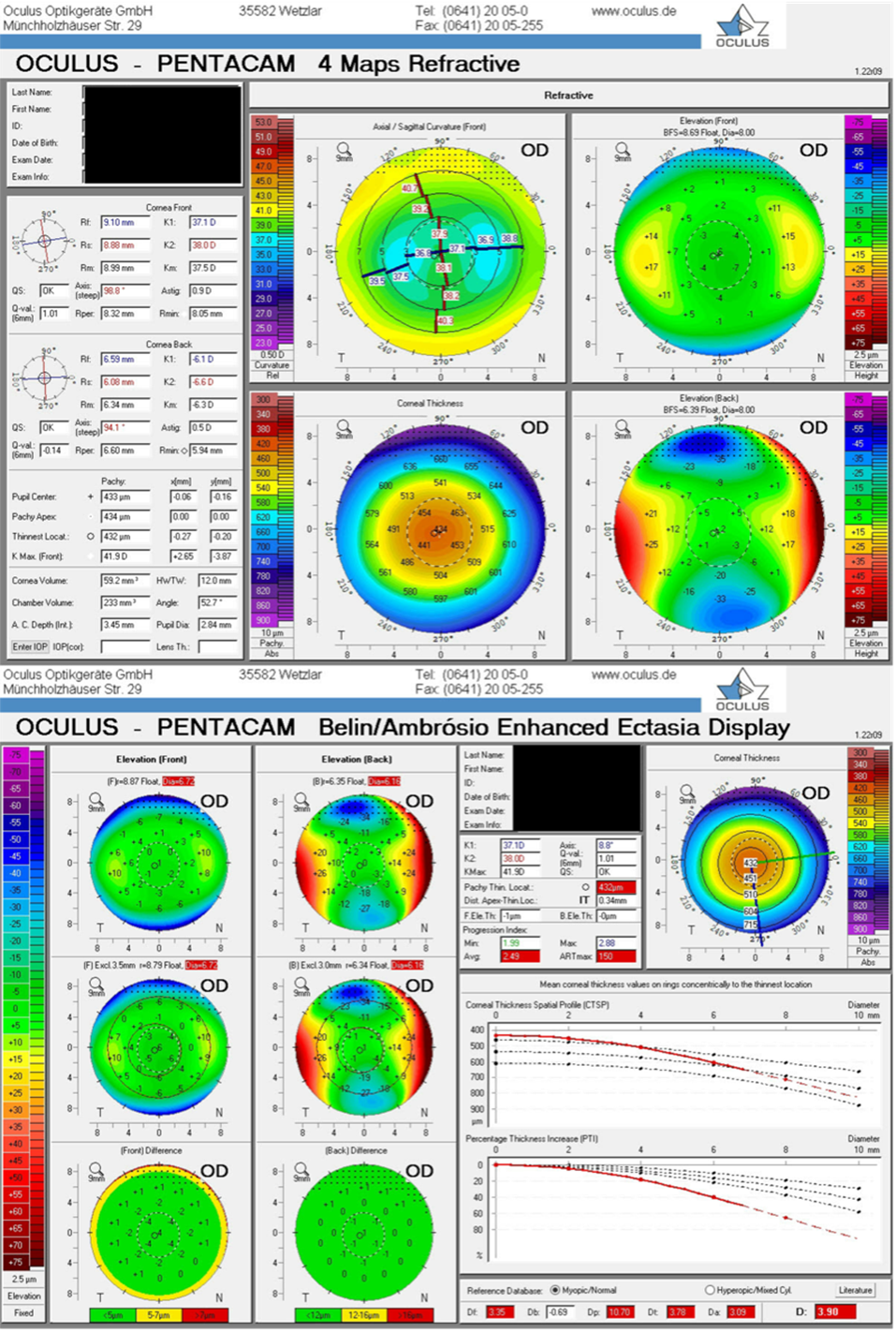
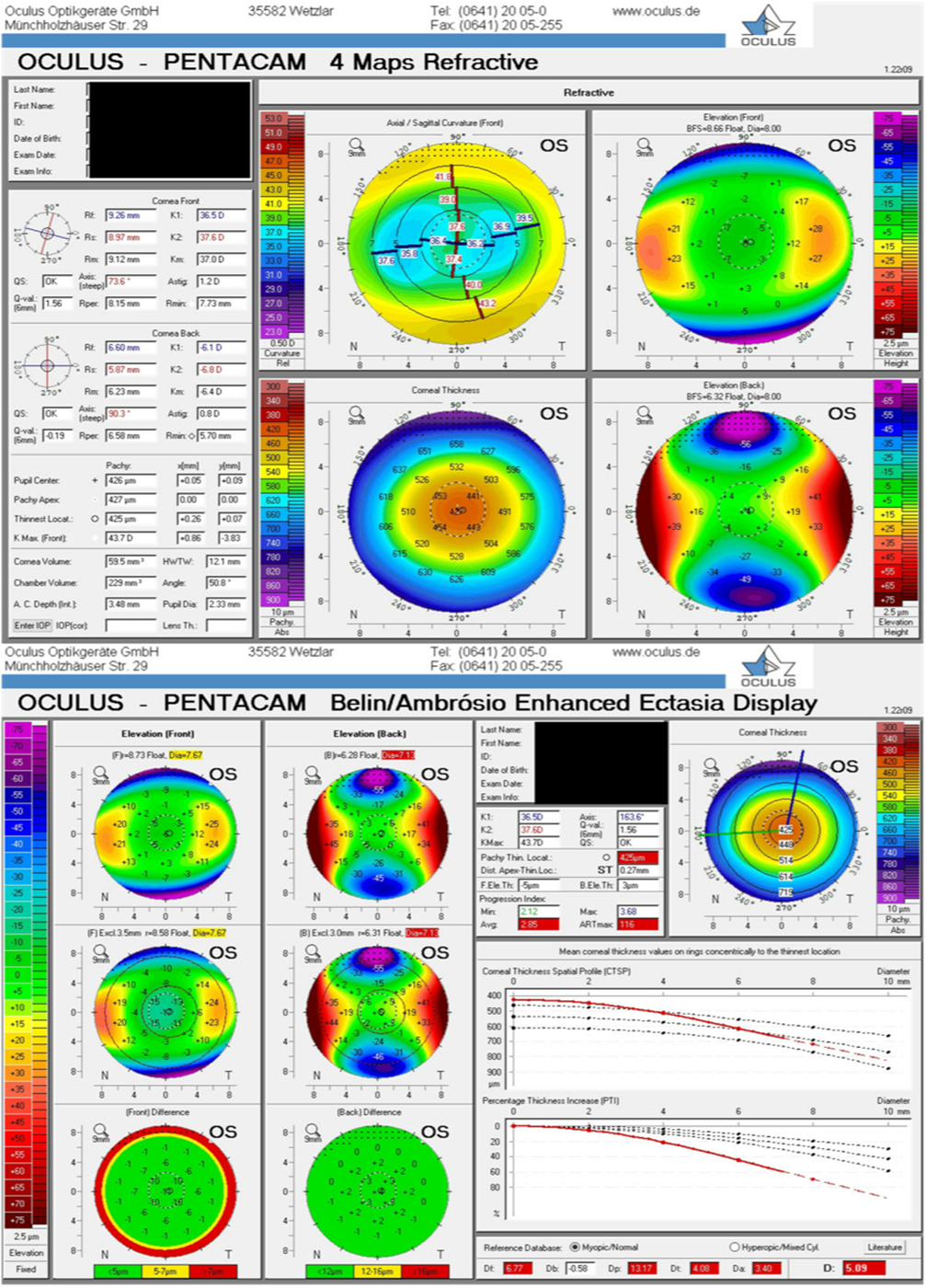
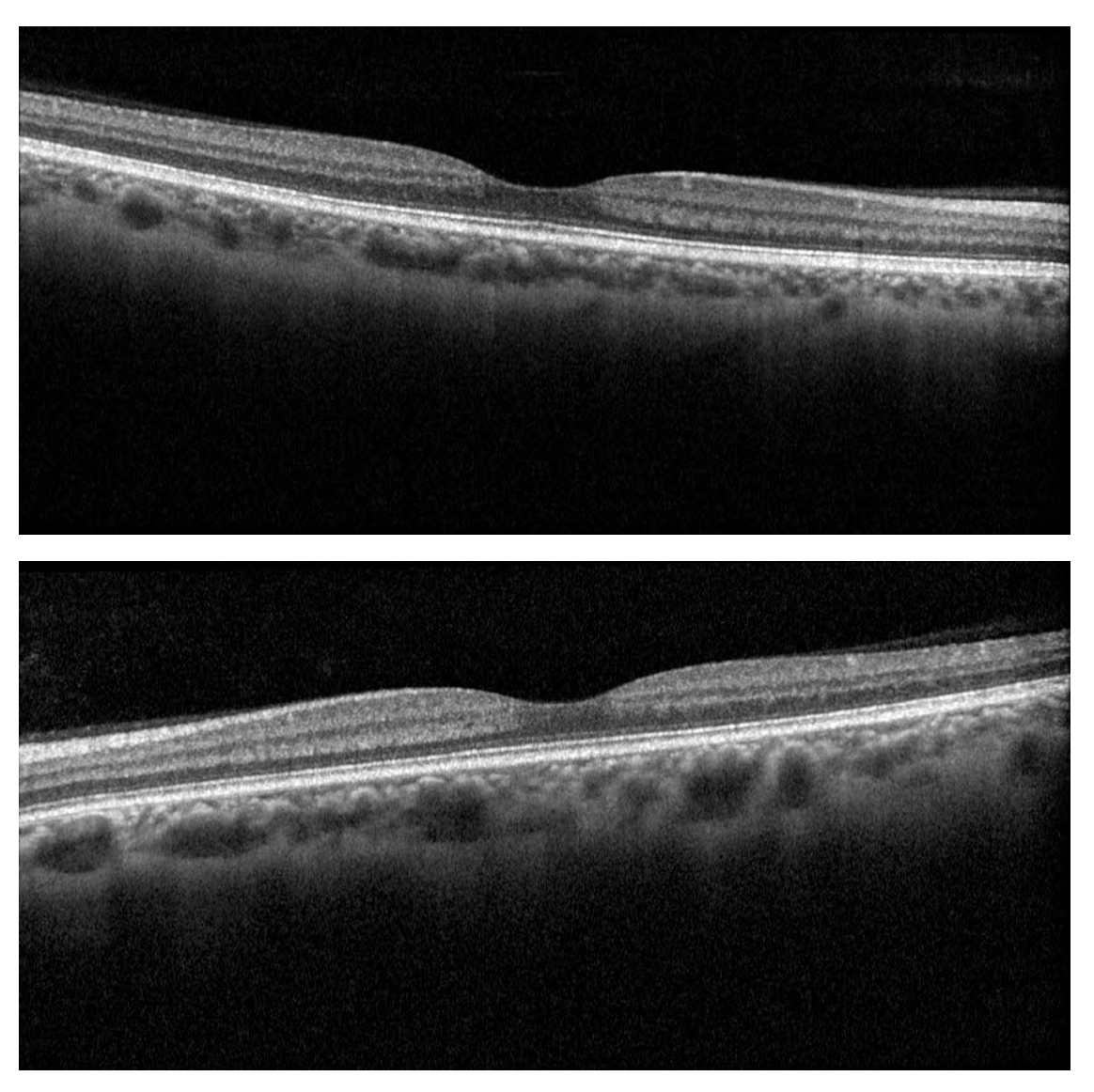
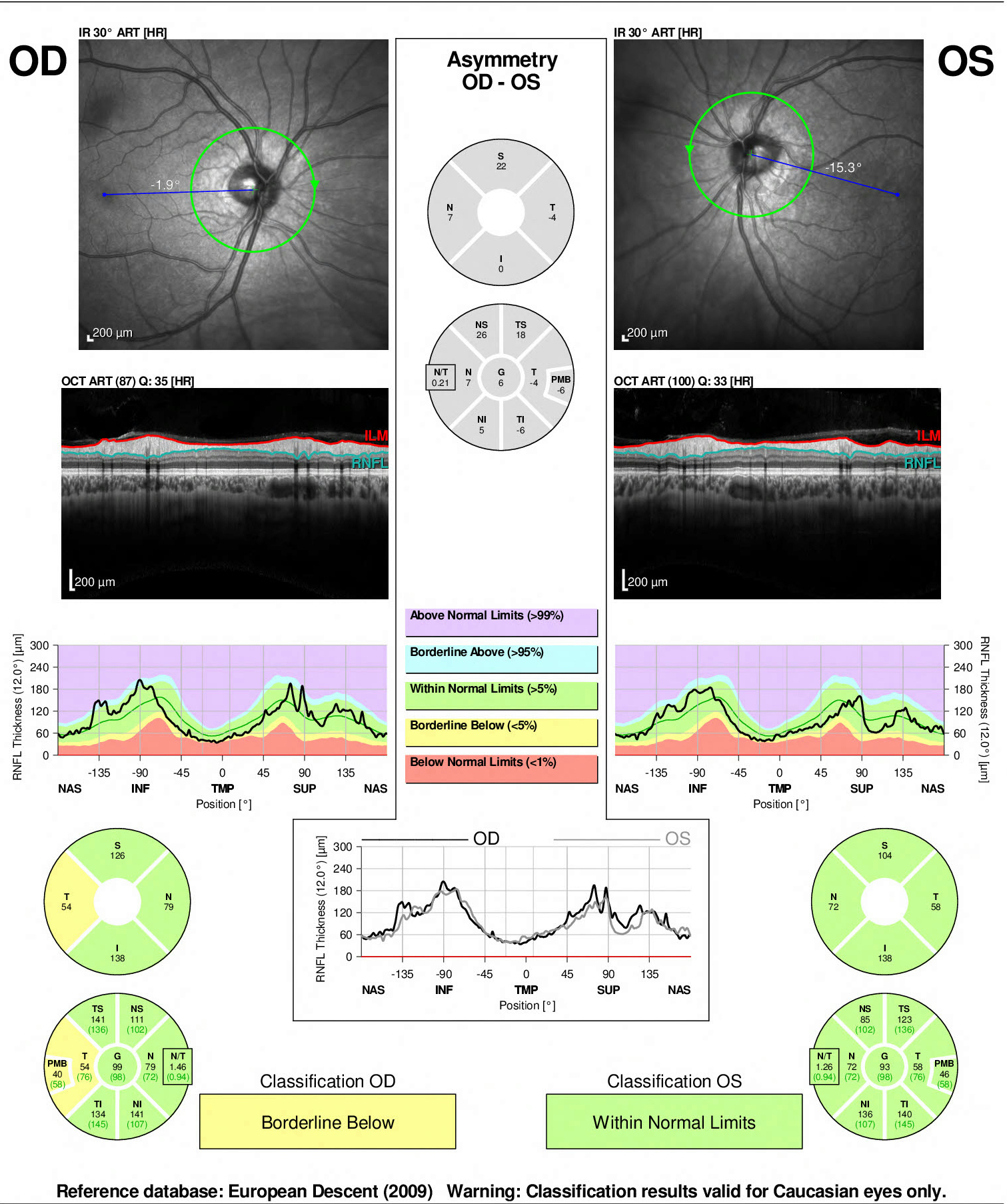
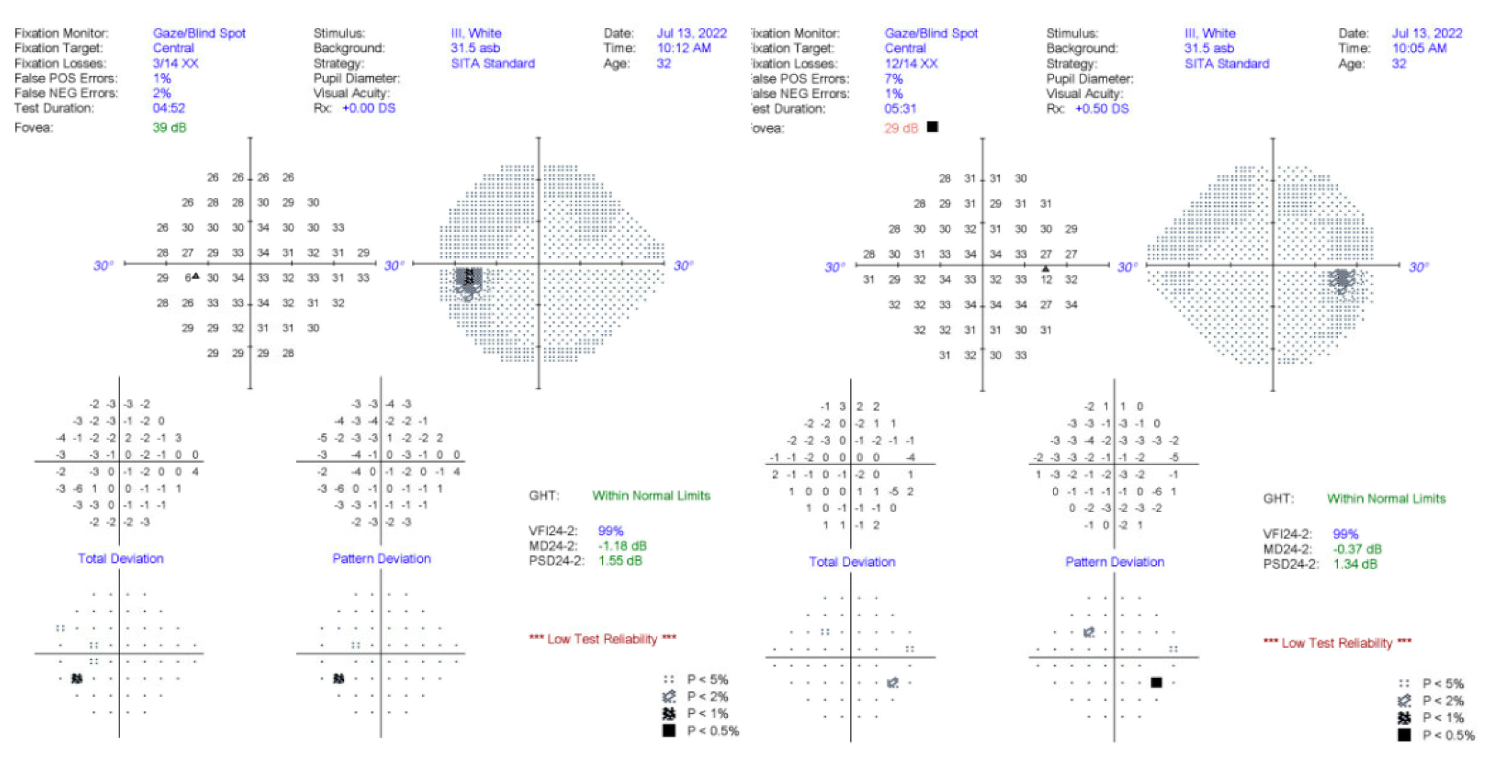
Corneal topography (Figures 2a and 2b) performed with the Oculus Pentacam revealed a typical post-LASIK cornea treated for myopia with central flattening. Optical coherence tomography conducted with the Heidelberg Spectralis optical coherence tomography depicted unremarkable maculae with normal foveal contours (Figure 3) and a normal retinal nerve fiber layer of the left eye and borderline thinning temporally in the right eye (Figure 4). Undilated perimetry was assessed using the Zeiss Humphrey Field Analyzer 3, which showed rare nonspecific and scattered defects in both eyes but was unreliable owing to fixation losses (Figure 5). No notable defects were discovered.


_and_left_eye_(bottom)_w.png)
_and_left_(right_side)_optic_nerves._.jpg)
_and_left_eye_(left_side)._low_test_rel.png)
With no overt ocular cause of the monocular diplopia, palinopsia, and photopsia, it was decided that the most probable cause of these visual disturbances was the topiramate. The prescribing neurologist was contacted, and a request was made to discontinue the medication. Because of the substantial improvement in migraines with the topiramate, the neurologist decided to continue the medication. Given this decision and no available treatment options to correct the visual disturbances, the plan was to follow up in 6 months. Several months later, the patient decided to self-discontinue the topiramate as she felt the visual disturbances were far more troublesome than the migraines. Within 1 week, the monocular diplopia of both eyes, palinopsia, and photopsia had completely resolved.
DISCUSSION
Topiramate is an orally administered anti-epileptic drug initially designed to treat epilepsy17 and then migraines.18 Later, it gained indication for other conditions such as bipolar disorder,19,20 eating disorders,21 alcohol and tobacco dependence,22,23 idiopathic intracranial hypertension,24 post-herpetic neuralgia,25,26 and tremors.27,28 Topiramate is a sulfa-derived monosaccharide with multiple mechanisms of action, including blocking voltage-gated sodium channels, blocking L-type calcium channels, augmenting post-synaptic gamma-aminobutyric receptor activity, modulating glutamate receptors, and mildly inhibiting carbonic anhydrase.29 It is rapidly absorbed and has a half-life of roughly 24 hours.29,30 The most recognized ocular risk is acute angle closure.31 Other ocular side effects include myopic shift, ciliochoroidal effusion syndrome, anterior uveitis, scleritis, vitritis, visual field defects, corneal thickening, diplopia, palinopsia, and Alice in Wonderland syndrome.31–35 Most, but not all, ocular conditions resolve after discontinuing topiramate.36
In the case of our patient, differential diagnoses included, but were not limited to, post-LASIK corneal ectasia or corneal irregularity, dry eye disease, opacification within the visual axis, or maculopathy. However, these etiologies were ruled out through examination and diagnostic testing. Corneal topography demonstrated no irregularities. Foundational dry eye disease treatment, in the form of preservative-free artificial tears and warm compresses, was initiated with no improvement in symptoms. Moreover, there were no signs of dry eye disease or tear film instability. Although there was a pinpoint spot of posterior subcapsular cataract in the left eye, this could not explain the visual disturbances in the right eye. Macular optical coherence tomography scans also revealed no structural abnormalities and normal foveal contours. Given the inability to explain such subjective visual symptoms through ocular findings, our attention turned to the central nervous system, as that seemed to be the next most likely origin. She had an essentially unremarkable brain magnetic resonance image, performed just before starting topiramate, to suggest that she had no structural lesion for the cause of her visual symptoms. Thus, a review of her medication list revealed the cause.
The visual disturbances of monocular diplopia, palinopsia, and photopsia occurred within 2 months of beginning topiramate and ceased within 1 week of discontinuing the medication. The patient took topiramate for a total of 10 months. Because there were no identifiable ocular causes or ocular changes observed, all vision changes were attributed to central nervous system disruptions related to topiramate. In other cases of topiramate-induced palinopsia, visual disturbance onset ranged from 1 month to 2.5 years after the initial dose.34 Interestingly, visual disturbances seem to occur independent of the prescribed dose and have occurred in dosages as low as 25 mg per day.35 These visual disturbances may occur because of dysfunction of the coordination system of the parietal lobes, inhibition of neural activity, or inability to inhibit motion streaking or may occur in people with a predisposition to slow visual processing in conjunction with topiramate, which is a central nervous system suppressant.35
CONCLUSION
Owing to the frequent use and broad spectrum of indications for topiramate, health care professionals such as neurologists, psychiatrists, ophthalmologists, and optometrists should be aware of the potential systemic and ocular side effects. Ophthalmic evaluation should include intraocular pressure assessment, refraction, fundoscopic examination, and perimetry. Although acute angle closure generally occurs within 2 weeks of the initial dose, visual disturbances may occur at any timepoint.36 Given the systemic and ocular side effects of topiramate, a multidisciplinary approach may be warranted when caring for patients taking topiramate when visual symptoms arise to quickly identify and appropriately manage any adverse effects. No identifiable health information was included in this case report.
Take home points:
-
Topiramate can result in visual disturbances including diplopia, palinopsia, and photopsia.
-
The condition is a diagnosis of exclusion and therefore additional testing is warranted.
-
Symptoms can fully resolve upon discontinuing the medication.
ACKNOWLEDGMENTS
I would like to thank Victoria Pelak, whom I consulted with during this case. It was her clinical judgment and experience that led to the recommendation of discontinuing the topiramate. I would also like to thank Kevin Abbott, who created Figure 1, which accurately depicted the palinopsia described and experienced by the patient.
CONFLICT OF INTEREST
The authors declare no conflicts of interest.