INTRODUCTION
The foramen ovale is an opening in the atrial septum between the two upper chambers of the heart, which is important in fetal development. Because fetal blood does not pass through the lungs for oxygenation, the foramen ovale allows blood to pass directly from the venous circulation of the right side of the heart to the arterial circulation of the left side of the heart. In most individuals, this hole closes at birth or shortly thereafter, but in approximately 25% of the general population, it remains at least partially open and is considered a patent foramen ovale.1
Although most individuals with a patent foramen ovale remain asymptomatic throughout their life, there is an association with patent foramen ovale and stroke. Due to this relationship, individuals with an unexplained, or cryptogenic, stroke, particularly those younger than age 55 without other stroke risk factors, need to have a patent foramen ovale ruled out with a bubble study.2,3 Although it is difficult to prove causation, in patients with stroke with a patent foramen ovale, the fewer traditional stroke risk factors present (hypertension, diabetes mellitus, vascular lesions, smoking), the greater the likelihood that the stroke is related to the patent foramen ovale.3
The exact mechanism for patent foramen ovale association with stroke is not completely understood. One possible explanation is that there is a paradoxical embolization of venous thrombi through the patent foramen ovale into the arterial circulation.4 More likely, there is a multifactorial association, with stroke risk related to size of the foramen ovale, presence of an atrial septal aneurysm, atrial anatomic variants, and hypercoagulable states.3
Most health professionals consider cerebral ischemia, or stroke, as a medical emergency, but not all view retinal ischemia with the same urgency. More recent studies have shown that patients with isolated retinal infarctions have an increased stroke rate.5,6 Current practice guidelines have been updated to consider any acute retinal ischemia, including transient ischemia, as the equivalent of a cerebral stroke; these must be treated with the same urgency of care.5,7
This case report demonstrates retinal ischemia secondary to a retinal artery occlusion in an otherwise healthy patient for whom work-up uncovered patent foramen ovale. Prompt diagnosis and management of both retinal ischemia and patent foramen ovale are critical to prevent additional central nervous system ischemic events. Current guidelines for management of retinal ischemia are discussed.
CASE REPORT
A 54-year-old woman presented for an urgent ophthalmic evaluation due to sudden loss of vision in the left eye. She reported noticing bright silver lights in her vision on awakening that morning. Later in the day, she covered her right eye and realized that she could only see a gray fog with her left eye. Review of systems was otherwise negative for eye pain, diplopia, headache, weakness, myalgias, jaw claudication, scalp tenderness, nausea, or change in appetite. Medical history was remarkable only for a past episode of vertigo several years prior. Specifically, she denied a history of hypertension, hypercholesterolemia, or diabetes mellitus. She was a former smoker, having quit 27 years prior.
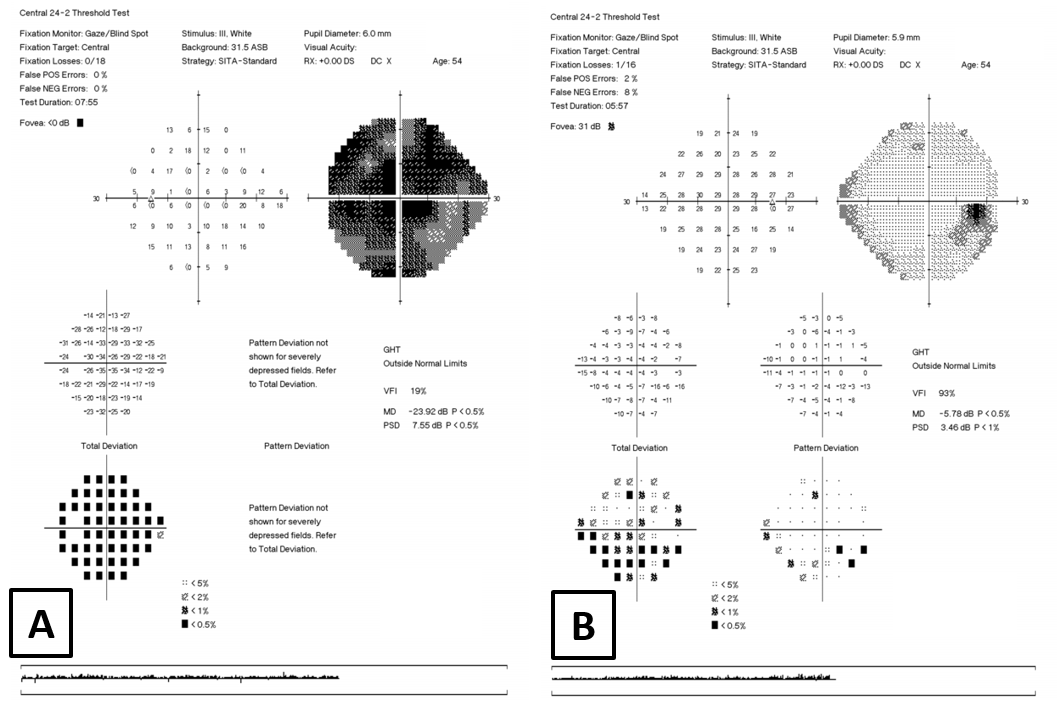
On examination, visual acuity was 20/20 in the right eye and 20/50 in the left eye. Pupils demonstrated physiologic anisocoria, with the right pupil 0.5 mm larger than the left pupil in both bright and dim illumination. Both pupils were equally reactive, with a 1.2 log unit relative afferent pupil defect in the left eye as measured with a neutral density filter. Color vision was reduced in the left eye only, correctly identifying only 2 out of 14 Ishihara color plates. Confrontational field testing was full to finger counting in both eyes, but red target testing uncovered cecocentral and superior nasal relative scotomas in the left eye. Automated 24-2 Humphrey Visual fields showed significant central and cecocentral field defects in the left eye (Figure 1). Ocular motilities were full, and all other aspects of the efferent visual system were unremarkable.
_left_eye---dense_central_and_cecocentral_defect.png)
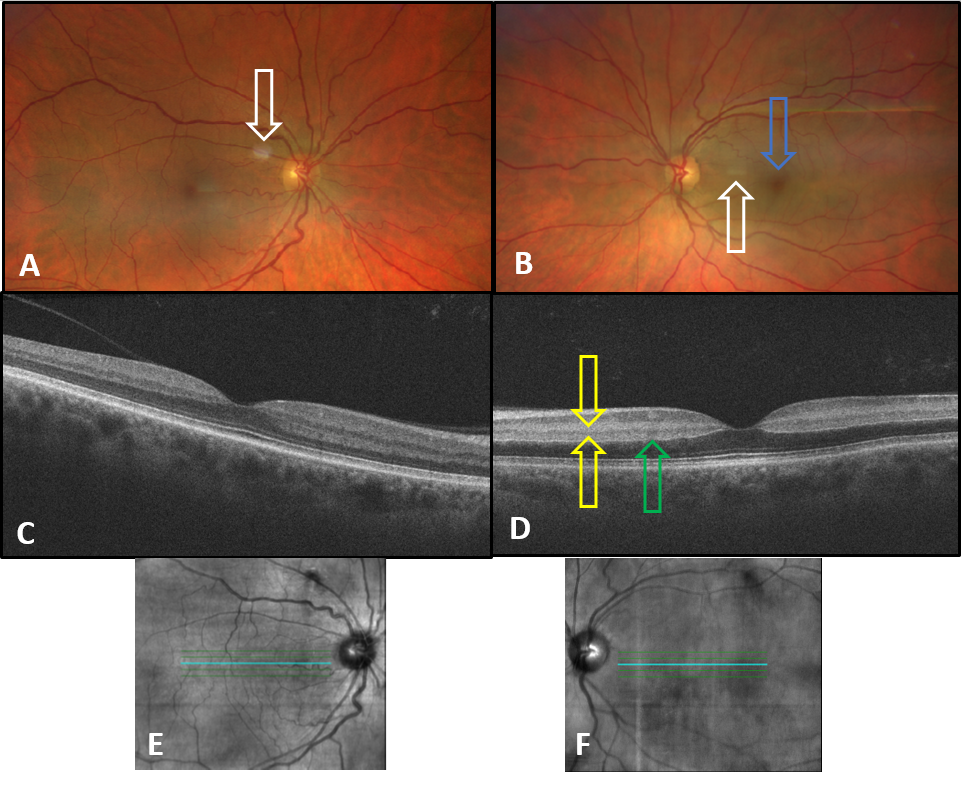
Blood pressure was measured as 152/92 mm Hg in-office, which the patient reported was uncharacteristic. Repeat measurement later that day in the emergency department triage was 123/62 mm Hg. Anterior segment was unremarkable, and intraocular pressures were normal. Results of dilated fundus examination of the right eye was normal. Fundus examination of the left eye showed retinal pallor in the area of the papillomacular bundle with a “cherry-red” appearance of the fovea. The remainder of the left retina and optic nerve head appeared perfused on clinical examination (Figure 2). Optical coherence tomography of the left eye showed hyper-reflectivity of the inner and outer plexiform retinal layers and middle retina edema in the macular region (Figure 2).
_fundus_photography_of_right_eye_showed_no_evidence_of_retinal_ischemia._camera_artifac.png)
Owing to the concern for an acute retinal artery occlusion, the patient was urgently referred to an emergency department with a dedicated stroke center for work-up. While hospitalized, she underwent noncontrast brain magnetic resonance imaging with diffusion sequencing and magnetic resonance angiography of the head and neck, which were all unremarkable. She was assessed for giant cell arteritis, myocardial infarction, and hypercholesterolemia and had extensive laboratory tests to assess for hypercoagulable states including prothrombin time, partial thromboplastin time, protein C function, protein S function, von Willebrand factor, antithrombin III, factor II prothrombin, plasminogen activator inhibitor, methylene tetrahydrofolate reductase, anticardiolipins, antineutrophil cytoplasmic antibody, beta-2 glycoprotein 1 antibody, and antinuclear antibody. All testing returned negative results. Etiology of the retinal artery occlusion was thought to be cryptogenic at this point, which prompted cardiac evaluation through transesophageal echocardiogram with bubble study. This revealed a 5-mm-diameter patent foramen ovale with left to right shunting, confirmed by a significant number of early bubbles in the left atrium with agitated saline testing. The patient was treated with aspirin 81 mg and clopidogrel 75 mg for 21 days and subsequently underwent successful outpatient percutaneous patent foramen ovale closure.
DISCUSSION
Acute retinal ischemia is characterized by sudden painless unilateral vision loss. Types of acute retinal ischemia include transient monocular vision loss of vascular origin, central retinal artery occlusion, and branch retinal artery occlusion.5 A cilioretinal artery occlusion is one type of branch retinal artery occlusion. Approximately 6.9%–49.5% of the population have a cilioretinal artery, which typically supplies the macular region of the retina.8
Episodes of transient monocular vision loss typically last several minutes, but can last an hour or more, and are characterized by complete visual recovery. In nontransient cases of acute retinal ischemia, the extent of vision and/or visual-field loss is dependent on which arteries are affected. Typically, a central retinal artery occlusion will have more severe and long-lasting visual consequences compared with a branch retinal artery occlusion, which usually only affects a portion of the visual field. In cases with an unaffected cilioretinal artery in the setting of a central retinal artery occlusion, central vision may be preserved. Conversely, an unaffected central retinal artery in the setting of a cilioretinal artery occlusion may result solely in central vision loss.
Although the diagnosis of acute retinal ischemia from transient monocular vision loss is ultimately made using patient history, retinal artery occlusions often have characteristic clinical findings. In some cases, depending on the extent of the retinal ischemia, a relative afferent pupillary defect will be present in the affected eye, along with potentially decreased acuity and color vision, as well as compromised visual fields. Fundoscopic examination findings may vary dependent on the artery occluded. In cases of central retinal artery occlusion, an embolus is not likely visualized on examination. The occlusion is likely where the central retinal artery enters the optic nerve dural sheath or possibly at the lamina cribosa.9 An acute central retinal artery occlusion is characterized by a pale white fundus with a cherry-red fovea, attenuated arteries, and “boxcarring” caused by segmental flow in the arteries. The optic nerve head remains perfused in an acute central retinal artery occlusion because of an alternate main blood supply to the optic disc, the short posterior ciliary arteries. Although the optic disc appears normal in an acute central retinal artery occlusion, it can later become pale and atrophic, as the central retinal artery supplies the inner retina where the axons of the ganglion cells travel before becoming the neuroretinal rim of the optic disc. A more posterior acute event, such as an ophthalmic artery occlusion, could result in combined retinal ischemia and optic disc ischemia/edema.
Branch retinal artery occlusion findings are similar to a central retinal artery occlusion but would only be found in the areas of the retina supplied by an occluded arteriole branch. In a cilioretinal artery occlusion supplying part of the macula, an area of retinal pallor would extend from the temporal portion of the optic nerve head to the macular area. The extent of the papillomacular bundle supplied by the cilioretinal artery is individual-specific, resulting in variable levels of vision loss and visual field defects in both cilioretinal artery occlusions and central retinal artery occlusions.10,11
Clinical findings are often sufficient to make a diagnosis of acute retinal artery occlusion and initiate an emergent referral to a stroke center, but additional diagnostic procedures can be considered to aid in the diagnosis. Fluorescein angiography showing a delay in the filling of retinal arteries and arteriovenous transit time has historically been the standard for diagnosis of retinal arterial occlusions. With the advent of optical coherence tomography, there is now a more readily available and noninvasive technology to assist in the diagnosis. On spectral domain optical coherence tomography, acute retinal ischemia typically exhibits retinal edema and hyperreflectivity of the inner retina.12 The optical coherence tomography may also show retinal middle layer opacification with findings characteristic of paracentral acute middle maculopathy and/or a prominent middle limiting membrane. Paracentral acute middle maculopathy is characterized by a hyperreflective band-like lesion in the inner nuclear layer that may extend to the outer plexiform layer.13 Paracentral acute middle maculopathy can be associated with many types of retinal vaso-occlusive disorders, including central retinal artery occlusion, branch retinal artery occlusion, and cilioretinal artery occlusion.14,15 In a study of 58 eyes with either an acute central retinal artery occlusion or branch retinal artery occlusion, almost 60% of eyes showed evidence of paracentral acute middle maculopathy on optical coherence tomography.13 In another study of 28 eyes with acute cilioretinal artery occlusion, 100% showed evidence of paracentral acute middle maculopathy on optical coherence tomography.16 A prominent middle limiting membrane appears as a hyperreflective line in the inner synaptic portion of the outer plexiform layer. Mangla et al. found that the presence of prominent middle limiting membrane was more characteristic of a mild or moderate acute central retinal artery occlusion rather than a severe central retinal artery occlusion.17 Abtahi et al. proposed the concept of a retinal ischemic cascade where paracentral acute middle maculopathy is considered the earliest form of retinal infarction that can have vertical progression to include the entire middle and inner portions of the retina.14
The optical coherence tomography in the case presented here shows evidence of both paracentral acute middle maculopathy and a prominent middle limiting membrane (Figure 2), consistent with the diagnosis of acute retinal ischemia. This is likely a presentation of a mild central retinal artery occlusion based on the fundus appearance and 20/50 visual acuity, but without confirmatory testing with fluorescein angiography, a branch retinal artery occlusion or cilioretinal artery occlusion cannot be ruled out.
In patients older than age 50, giant cell arteritis–associated arteritic retinal ischemia should be investigated. Based on a negative giant cell arteritis assessment in the hospital, this case likely represents a nonarteritic central retinal artery occlusion. The most common cause of nonarteritic retinal ischemia is thromboembolism from a distant source such as the internal carotid artery, aortic arch, or heart; these structures need to be carefully assessed.18 Table 1 includes additional etiologies of acute retinal ischemia to be considered.
Regardless of the type of acute retinal ischemia, whether it be in the form of transient monocular vision loss of vascular origin, branch retinal artery occlusion, central retinal artery occlusion, or cilioretinal artery occlusion, it should be treated as a medical emergency. The mechanisms that cause retinal ischemia are similar to those that cause cerebral infarction or stroke.5 Multiple studies have shown that patients with a history of a retinal artery occlusion have an increased risk of future stroke, myocardial infarction, or death.19–21 A systematic literature review with meta-analysis published in 2020 showed that 30% of patients with a central retinal artery occlusion and 25% of patients with branch retinal artery occlusion showed evidence of acute cerebral ischemia on magnetic resonance imaging completed within 7 days of the retinal arterial occlusion.22 The Retina and Ophthalmic Artery Occlusions Preferred Practice Guidelines published by the American Academy of Ophthalmology in 2019 state that ophthalmic artery occlusion, central retinal artery occlusion, and branch retinal artery occlusion can all be associated with life-threatening conditions. Owing to the high risk of ischemic stroke in cases of ocular arterial occlusion, a prompt referral to a stoke center for a medical evaluation is recommended.23 Thus, acute retinal ischemia should be managed with the same urgency as cerebral ischemia; it should be considered a medical emergency.5
As soon as an eyecare provider diagnoses acute retinal ischemia, the patient should be emergently referred to a stroke center. Additional diagnostic testing such as fundus photography, optical coherence tomography, fluorescein angiography, etc. may be considered to confirm diagnosis, but they should not delay the transfer to a stroke center.23 Eyecare providers should not be referring the patient back to the primary care provider or other specialist. The next step should be referral to the closest emergency department affiliated with a stroke center or rapid-access transient ischemic attack clinic.5
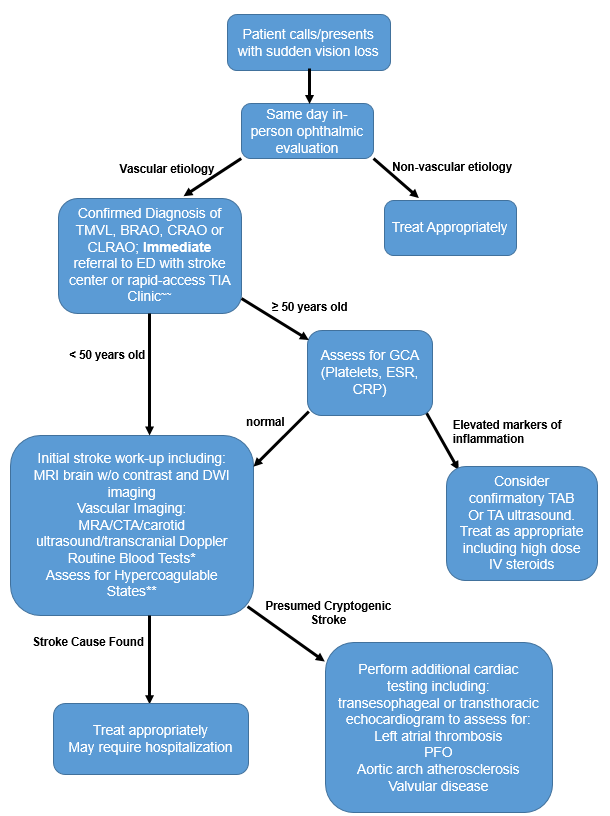
The recommended evaluation for acute retinal ischemia is outlined in Figure 3. Completion of an urgent brain magnetic resonance image with diffusion-weighted imaging is recommended to identify patients with a potential impending cerebral stroke so they can be stratified for immediate treatment and hopefully prevent additional stroke.5

If the initial evaluation of retinal ischemia or cerebral stroke does not reveal a cause and thus appears to be cryptogenic, further evaluation with transesophageal echocardiogram is warranted. These cardiac studies can help identify possible stroke etiologies such as a left atrial thrombus, aortic arch atherosclerosis, heart valve disease, septal aneurysm, or, as in the case presented here, a patent foramen ovale. A prospective study included 485 patients with acute retinal or cerebral ischemia. Routine stroke work-up (including hypercoagulable studies) did not determine an etiology and thus were considered cryptogenic in 67.8% of patients. The addition of transesophageal echocardiogram testing led to a possible etiology in 48.4% of these patients. In patients younger than 55 years, such as presented in this case, isolated patent foramen ovale was detected in 24.4%, and patent foramen ovale with atrial septum aneurysm was detected in 20.9% of patients with previously classified cryptogenic stroke.24
Patent foramen ovale diagnosis is typically done with either transthoracic echocardiography or transesophageal echocardiogram, both with a bubble study.25,26 The studies look for right-to-left shunting that would be consistent with a patent foramen ovale. Transcranial Doppler ultrasonography is often used in conjunction with transesophageal echocardiogram to make a diagnosis.26
The treatment of patent foramen ovale has been under debate. Because patent foramen ovale can be an incidental finding, it can be difficult to link the cause of an otherwise cryptogenic stroke to patent foramen ovale. More recently, several studies indicate that, in select individuals, closure may be the preferred treatment over medical management. A meta-analysis of multiple randomized clinical trials in patients with patent foramen ovale and cryptogenic stoke showed that percutaneous closure of patent foramen ovales reduces the risk of recurrent stroke compared with medical management with antiplatelet or oral anticoagulation therapy.25,27 The general consensus is that patients with high-risk patent foramen ovale features who are younger than age 60, with no other mechanism for stroke identified, should be recommended for percutaneous closure.26
Most patients with cryptogenic stroke would likely be treated with blood thinners to reduce future stroke risk. However, despite this treatment, those with an undiagnosed patent foramen ovale could remain at unnecessary increased risk of recurrent stroke or other neurological event. This emphasizes the importance of investigating for patent foramen ovale in patients with cryptogenic stroke, including those presenting with retinal ischemia, with no identified alternate etiology after initial stroke work-up.
CONCLUSION
Any form of acute retinal ischemia, including transient monocular vision loss, is considered on par with stroke and necessitates urgent referral to a stroke center or a rapid access transient ischemic attack clinic. For cases in which a causative etiology for ischemic embolic stroke or any retinal artery occlusion cannot be explained by any other probable cause, it is important to consider and evaluate for patent foramen ovale. Because patent foramen ovale is common, occurring in approximately 25% of the general population, eye doctors need to be aware of the possible association of patent foramen ovale and retinal ischemia and be sure their patients are screened in this regard as appropriate. No identifiable health information was included in this case report.
Acknowledgements
We thank Kelly Seidler, OD (Johns Hopkins Wilmer Eye Institute), for her assistance in the examination of the patient in this case report.
Take Home Points
-
Any acute retinal ischemia whether it be in the form of transient monocular vision loss, branch retinal artery occlusion, or central retinal artery occlusion should be treated as a medical emergency with prompt referral to a stroke center or rapid-access transient ischemic attack clinic.
-
In-office testing, such as optical coherence tomography, fundus photography, and fluorescein angiography, can be done to aid in identifying the retinal ischemia, but should not delay the emergent referral for a stroke evaluation.
-
If following acute retinal ischemia, a stroke evaluation including neuro-imaging and evaluation of inflammatory and hypercoagulable states is unrevealing, further testing for cardiac etiologies, such as a patent foramen ovale, should be completed.