Introduction
Retained natural and foreign materials may be discovered in the anterior, middle, and or posterior chambers of the eye following any penetrating injury or penetrating surgical procedure. Following cataract surgery, the commonly seen retained objects are remnants of uncollected lens material; however, other things such as cilia, suture material, or other debris from the surgical field are plausible. These objects may produce the following: (1) no signs or symptoms; (2) inflammation from allergens resting on the object; (3) inflammation based on the allergenic response to the object itself; or (4) infection from microorganisms resting on the object. These reactions may be suppressed and eliminated by the effects of both the preoperative and postoperative topical medicinal regimen (topical antibiotic, topical steroidal anti-inflammatory, and topical nonsteroidal anti-inflammatory).
Case Report
A 64-year-old African American woman presented for a 1-month postoperative examination following right eye cataract surgery. She was compliant with her pre- and postoperative care and had finished all of her topical postoperative medications. She reported seeing well and had no symptoms of lost function or pain. She denied trauma, history of systemic diseases, or allergies of any kind.
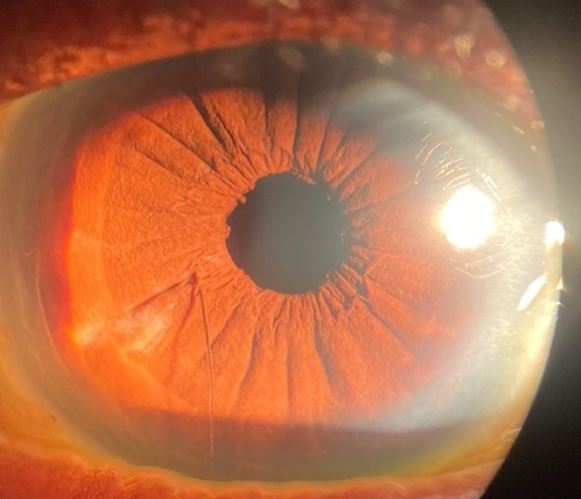
Her best-corrected entering visual acuities were 20/20 in her right eye and 20/20 in her left eye at distance and near through a refraction of plano in both eyes at distance and +3.00 D sphere at near. Her external examination was unremarkable with normal extraocular motilities, normal confrontational visual fields, and no evidence of afferent pupillary defect. Biomicroscopic examination of the right eye uncovered a single retained cilium in the anterior chamber (Figure 1).

There was no evidence of inflammation or infection (no cell/flare/hypopyon). Biomicroscopy of the left eye revealed a clear, well-centered posterior segment intraocular lens. Goldman intraocular pressures measured 14 mm Hg, in both eyes. Her undilated 90 D posterior segment findings were normal for both eyes, with normal nerves with small cups and quiet retinas with no macular pathology.
The diagnosis was an iatrogenically retained foreign body (cilium), following uncomplicated phacoemulsification with intraocular lens implantation in the right eye. In the setting of the absence of inflammatory or infectious signs, symptoms, or loss of function, a plan of monitoring was developed (6-month intervals), educating the patient to return immediately should adverse signs or symptoms (redness, lost vision, pain) begin.
Discussion
Retained natural and foreign materials may be discovered in the anterior, middle, or posterior segments of the eye following any penetrating injury or surgical procedure.1–3 These phenomena are commonly seen following traumatic globe rupture. Iatrogenic foreign body in the anterior chamber following cataract extraction may result from retained remnants of uncollected lens material, “implanted” cilia, a cilium that “self-inoculates” via interaction with one of the created wounds, suture material, or other debris from surgical instruments or the surgical field.1–4 Iatrogenic “intraocular foreign bodies” have been documented to produce variable ocular comorbidities.1,2 Patients may present asymptomatically or with unexplained painful visual interruption secondary to spontaneous corneal edema, intraocular inflammation, raised intraocular pressure, cystic macular edema, and endophthalmitis.1–4
Pathophysiology
The purpose of an immune response is reparative and protective.5,6 The eye is regarded as an “immune privileged” site.5,6 This term refers to the immunosuppressive and anti-inflammatory mechanism, which is mediated by resident ocular cells residing in tissues, the aqueous humor, and the anterior chamber.6 This evolutionary architecture assists in preventing unnecessary and unwanted damage to the eye, which, via an aggressive infiltrating inflammatory reaction, might otherwise create large-scale tissue disorganization leading to lost function (permanent visual loss or blindness).5,6
The properties of immune privilege make it possible for the eyes to regulate the intraocular innate and adaptive immune responses.1–8 This permits reduced rates of rejection for ocular transplanted tissues over extended periods of time.6 In contrast, other body sites have a high affinity for rejecting such transplants and grafts.6
To achieve immune privilege, the eye has multiple mechanisms that allow it to regulate potentially sight-threatening inflammatory responses.6–9 One of the mechanisms that creates peripheral tolerance to eye-derived antigens is known as the “anterior chamber-associated immune deviation.”6,8,9
Antigenic materials that invade the anterior chamber generate a systemic immune response that creates clonally expanded regulatory T-cells and B-cells that secrete large concentrations of immunoglobulin A.6–9 This is a non–complement-fixing antibody.6–8 The process is guided by regulatory T cells and ocular resident cells, which include corneal endothelial cells, ocular pigment epithelial cells of the anterior uvea and retina.6–8 There is also innate immune support from the aqueous humor itself.6–8
The reaction of an eye to a cilium is unpredictable, ranging from nothing to endophthalmitis.4,6,10 However, a cilium in the anterior chamber often remains inert.4,5,10–19 When a cilium enters the anterior chamber, the antigen presenting cells that become immunotolerant following exposure to naturally occurring transforming growth factor β in the anterior chamber engulfs the cilium.6–9 The now immunotolerant antigen presenting cell leaves the anterior chamber through the trabecular meshwork, moving into the bloodstream, where it travels to the spleen to initiate the generation of regulatory T cells.6–9 Two populations of these immunoregulatory cells consist of regulatory CD4+ T cells (the afferent regulators), capable of suppressing the initial activation and differentiation of naive T cells into Th1 effector cells, and regulatory CD8+ T cells (efferent regulators), capable of inhibiting the local expression of Th1-mediated immune responses, such as delayed hypersensitivity, at the local site.6,8,9 These regulatory T cells secrete immunosuppressive cytokines such as transforming growth factor β, which promotes the generation of non–complement-fixing antibodies such as immunoglobulin A.6–8
Furthermore, the regulatory T cells induced by ocular pigment epithelial cells, which constitutively express the transcription factor Foxp3, are indispensable for immune tolerance and homeostasis.6,9 They aid in the suppression of excessive immune responses that may be harmful to the host’s intraocular microenvironment.6,9
In contradistinction, materials “not of the body” introduced to the eye such as plant or organic matter, metals, or wood typically produce swift, severe complications such as nongranulomatous and granulomatous uveitis, epithelial iris cysts (keratin pearl cyst), cataractogenesis, corneal edema, sympathetic ophthalmia, and endophthalmitis via the cellular immune system.4–8,10 Acute inflammation/infection as a response to an offending allergen or microbe commonly begins within days to months of inoculation/introduction. In contradistinction, by personal experience and supported by the literature, eyelashes and cortical remnants are often tolerated for years without an adverse response.5,9
It can be hypothesized that there was another reason why the iatrogenically introduced eyelash remained inert during the postoperative cataract extraction healing period. Although the eyelash may have introduced allergens or microbes (normal flora) into the anterior chamber, the immune reaction may have initially masqueraded as part of the postoperative surgical inflammatory response. In addition to natural physiology, this process was already being suppressed and neutralized by the effects of the pre- and postoperative regimen of topical antibiotic, topical steroidal, and topical nonsteroidal anti-inflammatory medications.
Today, most cataract surgeons deploy topical antibiotic and topical non-steroidal anti-inflammatory agents 3 to 7 days preceding the procedure to reduce the risk of the postoperative infection and postoperative retinal inflammation (cystoid macular edema Irvine- Gass syndrome).10,11 These agents may have provided an immune regulatory prophylaxis that reduced inflammatory exaggeration secondary to this peculiarity.10,11
Diagnosis/Differential Diagnosis
Because a cilium was identified by direct observation, a differential diagnosis list is unnecessary.
Management
Removal of a retained eye lash is controversial. Some maintain a posture that no intervention is required in the absence of infection or lost function.4–9,12–19 Others prefer a preventive approach (especially when the location of a lash makes access to it easy, not requiring a trip to the operating room). The personal preference of an operating physician, even in quiet eyes, may opt for immediate removal to lessen the risk of future complications and late endophthalmitis.8,12–19
If it is decided that the lash is well placed so as to facilitate an uncomplicated biomicroscopic removal, a small, self-sealing corneal incision can be created adjacent to the lash’s vertical border. This is followed by viscoelastic dissection of the cilium from the iris surface. The procedure is completed with subsequent eyelash removal via sterile forceps.4 So long as the endothelium is undisturbed, the prognosis has an excellent record.
Following the procedure, topical fluorinated quinolone antibiotic drops four times a day along with topical steroid drops (prednisolone acetate 1%) four times a day and over-the-counter oral pain medication (acetaminophen or ibuprofen) can be prescribed as necessary for 7 days to prevent postoperative infection, hasten recovery from inflammation, and mitigate residual discomfort.10,11 Follow-up evaluation to ensure appropriate healing should occur 1 day after the procedure to ensure that there are no adverse or idiosyncratic reactions and that no endophthalmitis is evolving. A final follow-up visit can be scheduled for 7 to 10 days after surgery. The patient should be instructed to return to the office immediately should the eye present with increased redness or become more painful or if vison becomes reduced in either eye (sympathetic ophthalmia).
Conclusion
This patient was not having any difficulties, so it was decided by the surgeon to approach things conservatively, monitoring her recovery by educating the patient about the signs and symptoms of decompensation and reevaluating the situation at regular biannual intervals; the cilium will be removed immediately if signs or symptoms arise.
Retained natural and foreign materials can be deposited in the anterior, middle, or posterior chambers of the eye following any penetrating injury or surgical procedure. The anterior chamber is a common location for retained lens remnants that were too risky to remove during cataract surgery; although rare, other things such as cilia, suture material, or debris from the surgical field can be incarcerated as well. These objects may be discovered serendipitously, evoking no signs or symptoms and producing no inflammation, infection, or loss of function. Management (removal or monitoring) is based on the combination of the personal preference of the surgeon and the observable clinical picture.
Take Home Points
- Retained intraocular foreign bodies, such as cilia, can be found in the anterior chamber after a penetrating injury or intraocular surgery.
- The inflammatory response to these foreign bodies can vary widely, ranging from endophthalmitis to no response.
- Management options range from surgical removal to non-interventional monitoring based on the presence or absence of an inflammatory reaction to the foreign body.
- If the foreign body is inert, patient education and monitoring is an acceptable management option.