INTRODUCTION
Scleral lenses (SLs) vault over the cornea and land evenly onto the sclera and overlying conjunctiva allowing for correction of irregular astigmatism. Due to the fluid reservoir that is created between the scleral lens and the ocular surface, SLs have been used for rehabilitation of the ocular surface.1,2 Prescribing of SLs has increased from when they were first utilized in the 1800s due to accessibility of lens materials, lens designs, diameters, and advanced customizations. In addition, technological innovations have been instrumental in allowing practitioners to customize SLs and improve landing zone alignment, particularly for patients with irregular scleral shapes.3–9
Previous studies have described the ocular surface shape, providing practitioners with an evidence-based approach to SL fitting and evaluation.10–12 When practitioners first began to fit SLs, there were limitations with early lens designs. Most diagnostic SLs were fit with spherical landing zones, which was often not a problem when fitting a small diameter scleral lens (<15.6 mm). However, spherical landing zones made fitting patients with significant elevation differences and conjunctival irregularities difficult.5,10 More recently, there have been significant advances in lens design customizations and ocular surface imaging to improve SL fitting, minimizing the physiological effects such as corneal hypoxia, increased intraocular pressure, and conjunctival compression of the lens on the eye.13–15
Research has provided practitioners with a better understanding regarding the physiological and anatomical variations of the cornea in patients including corneal thickness, biomechanics, and endothelial cell morphology.13 Many patients do not have a spherical sclera and would benefit from advanced, nonspherical SL designs.13,16,17 A total of 140 eyes were studied utilizing the sMap3D profilometer (Cedar Crest, NM) by the Scleral Shape Study Group. They found that 95.3% of patients had a toric or asymmetric scleral while very few (5-6%) had a spherical sclera.13,16,17 Thus, corneoscleral profilometry may supplement the traditional method of fitting sclerals from diagnostic fitting sets, especially for patients with significant scleral toricity.
Profilometry-guided SL may ultimately improve patients’ comfort and quality of vision.10 Decentered lenses or those with inadequate corneal clearance may induce astigmatism and higher order aberrations, thus reducing vision.18 This case report will review the utilization of a profilometry-guided SL design to enhance comfort, vision, and landing zone alignment for a patient with high cornea and scleral toricity.
CASE REPORT
A 42-year-old patient was referred for contact lens fitting for vision improvement of her right eye. Her medical history was unremarkable. She denied history of trauma and infection. The patient reported a history of amblyopia. She did not have any allergies to medications, nor was she taking any systemic medications. Her last medical examination was 3 months prior. Entering corrected visual acuities with her habitual glasses were right eye 20/250, pinhole 20/80, and 20/20 left eye.
Entrance testing was unremarkable: pupils were equal, round, and reactive to light in both eyes without afferent pupillary defect. Confrontation fields and extraocular muscle testing were normal in both eyes. Intraocular pressures were 14 mmHg right eye, 16 mmHg left eye. Manifest refraction revealed a hyperopic and astigmatic anisometropic prescription of +5.50-8.00 x 160, 20/60-3 for her right eye and +0.50-1.25 x 175, 20/20 for her left eye.
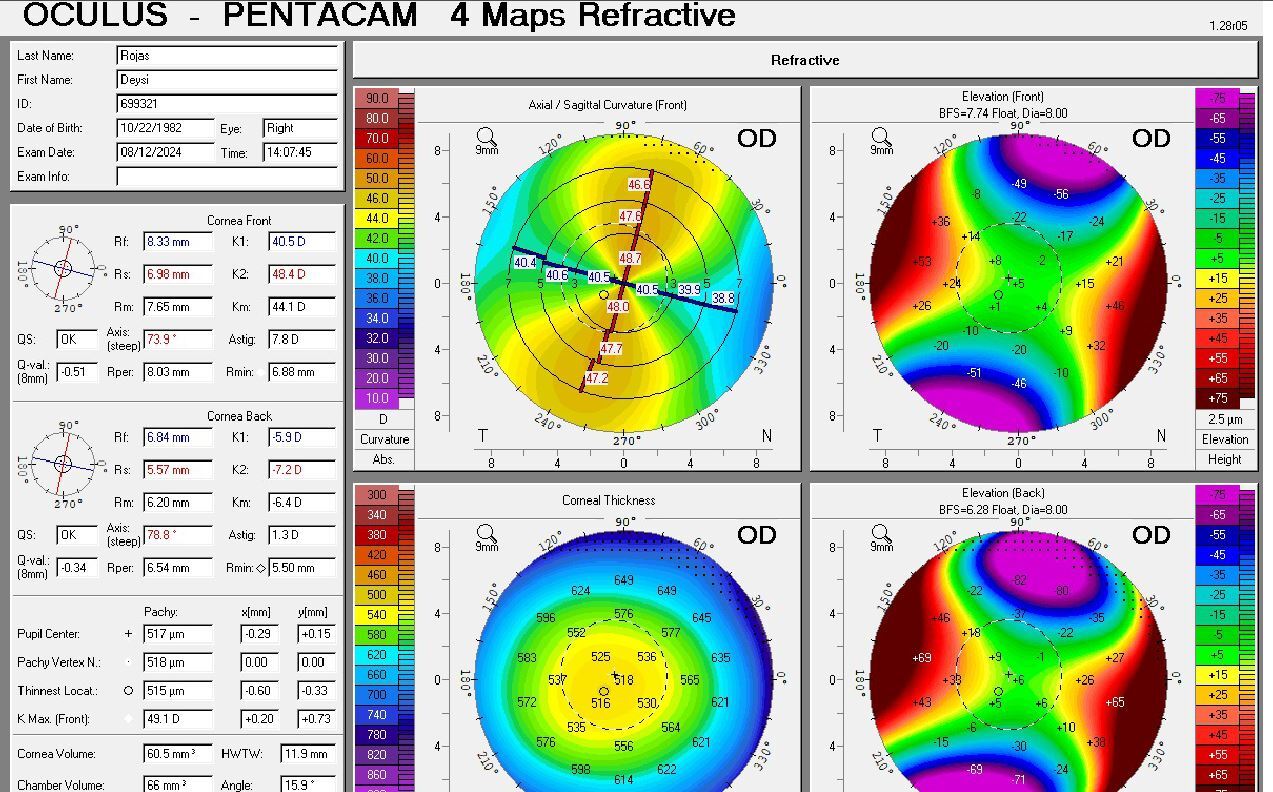
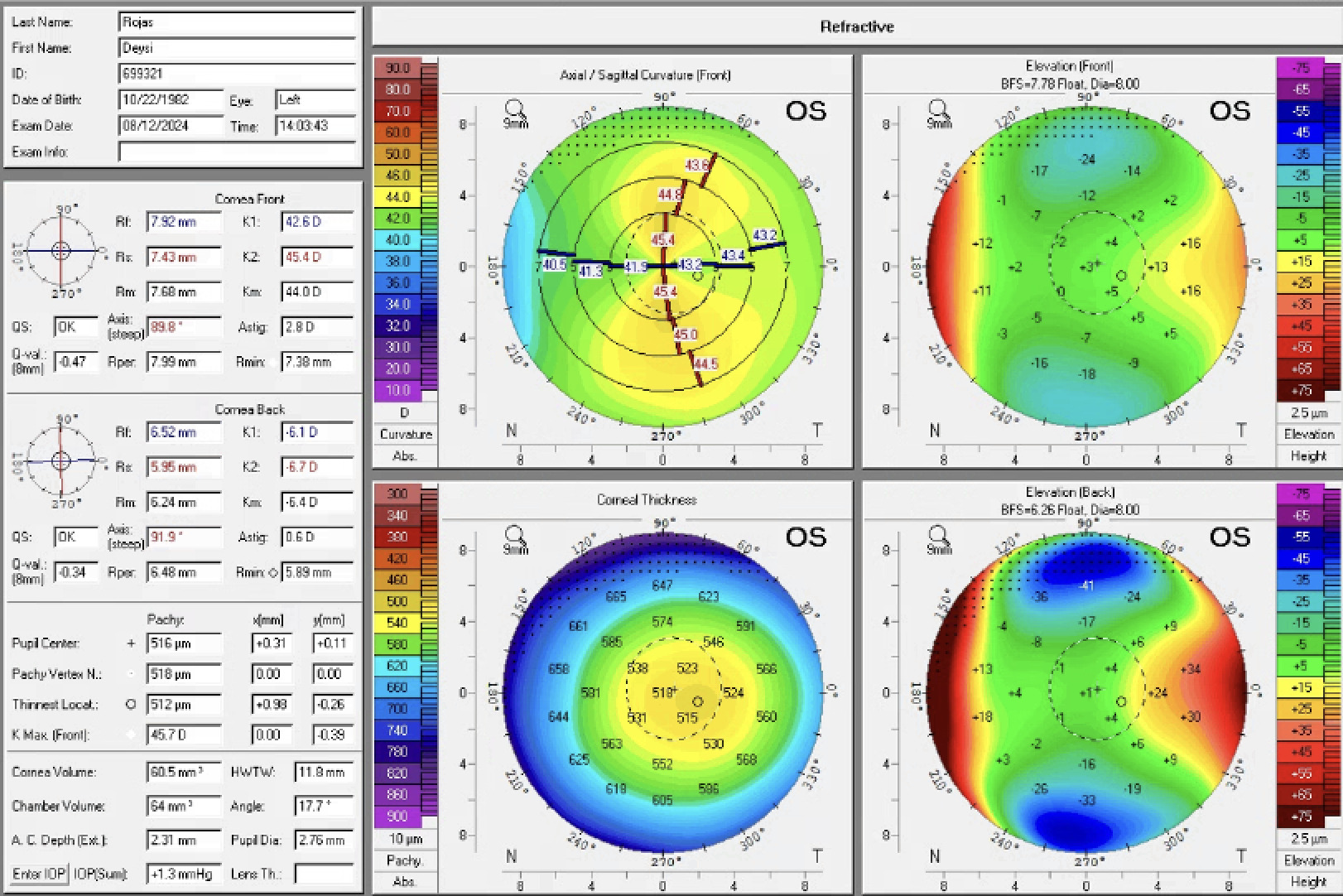
Slit lamp examination was unremarkable; there were no significant findings on the lids, cornea, or conjunctiva of either eye. Her angles were grade 2 nasally and temporally for both eyes, open to trabecular meshwork with gonioscopy. Fundus examination findings were normal. Corneal tomography scans (OCULUS Pentacam®, OCULUS Optikgrate GmbH) were performed on each eye due to the patient’s high astigmatism. Tomography scans revealed almost 8 diopters of limbus-to-limbus corneal astigmatism for her right eye (Figure 1a) and 2 diopters of regular corneal astigmatism for her left eye (Figure 1b).
_shows_high_limbus-to-l.jpg)
_shows_regular_with-the-.png)
Several contact lens designs were considered and discussed with the patient. A custom soft toric lens was considered as an option as it would provide good comfort. However, due to the amount of astigmatism of her right eye and only the slight improvement in acuity with refraction, soft contact lens optics were not expected to provide substantial visual benefits. As one of the patient’s main concerns was vision improvement, this option was therefore not pursued.
Hybrid and corneal gas permeable lenses could both have been used to determine best corrected vision, but due to the high limbus-to-limbus corneal astigmatism, there was concern that any lens on the right eye would provide unstable vision and fitting. After further consideration, it was determined that a scleral lens was preferred to improve vision. Scleral lenses vault over the ocular surface, generating a space between the anterior cornea and the back surface of the lens. This space is known as the fluid reservoir. The fluid reservoir is filled with non-preserved saline solution that supports the scleral lens, prevents corneal desiccation, and provides optical neutralization of aberrations from corneal surface irregularities. Scleral lenses are fit based on the principle of sagittal height. The sagittal height of the ocular surface is the maximum distance from a defined chord perpendicular to the ocular surface.2
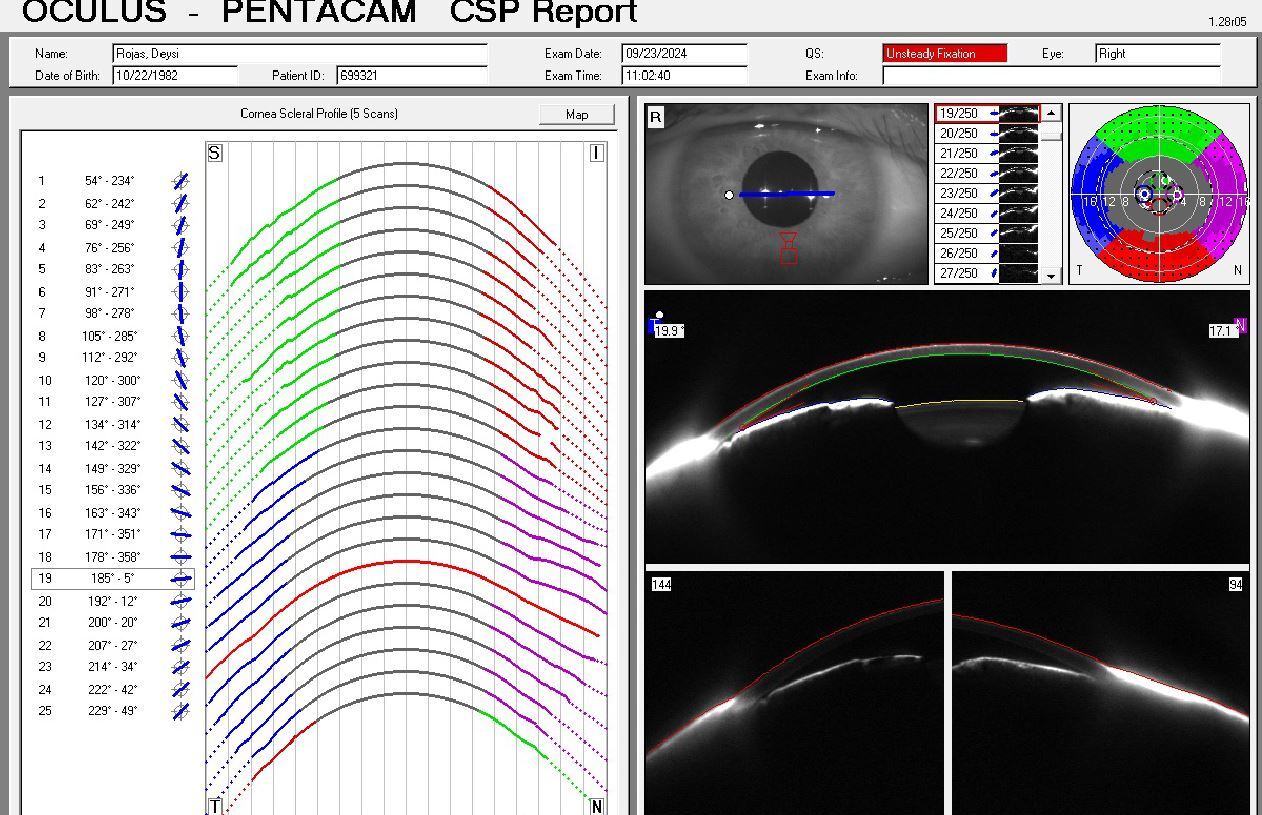
Initially, a diagnostic scleral lens diameter of 15.2 mm was selected as the patient had small (8.0 mm) interpalpebral apertures. However, this lens with 300 microns of toricity in the landing zone would not stay on the eye and became dislodged immediately after lens application. Next, a large diameter scleral lens with a toric landing zone and a specialized design where the lens has different sagittal depths in the vertical and horizontal meridians to match the asymmetric, nonspherical shape of the sclera was selected. This lens design was selected to try to obtain better alignment and lens stability because the smaller diameter lens demonstrated low central corneal clearance and higher edge lift. Larger diameter lenses often provide improved corneal and limbal vault for corneas with higher irregularity. Lenses with dual sagittal depths may also enhance stability by better aligning the distribution of the tear reservoir with the ocular surface. Following the fitting guide, the diagnostic lens applied to the eye had the following parameters: base curve 6.90, power -2.00, and overall diameter 17.0 mm. This lens showed significant edge lift off in the vertical meridian as soon as she looked in primary gaze after lens application. The patient also had a very shallow or flat low-profile ocular surface sagittal depth from the cornea to the sclera as well as narrow angles when viewed with Scheimpflug imaging (Figure 2). The lens was manually held in position to evaluate the central fluid reservoir depth and appeared to be double the thickness of the lens thickness. Corneoscleral profilometry was performed with OCULUS Pentacam® CSP (Cornea Scleral Profile) to determine if corneoscleral elevations and asymmetry were the cause of the SL misalignment.

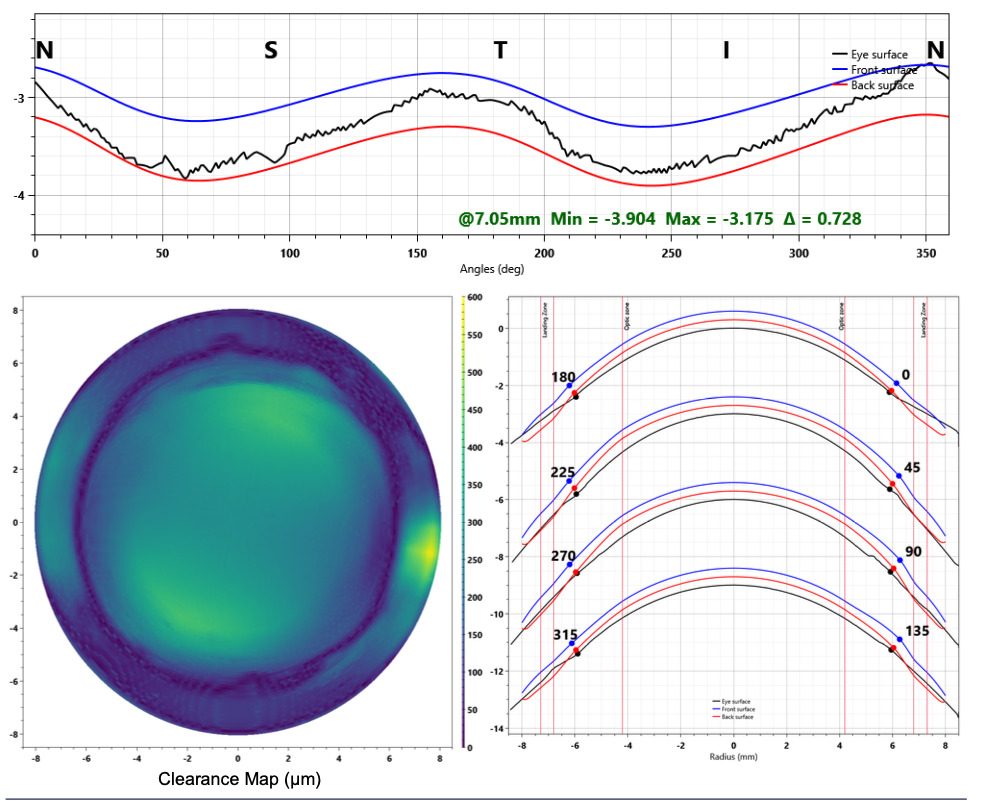
Corneoscleral profilometry with the OCULUS Pentacam® CSP was performed and 2 examiners were needed to acquire this patient’s scans, one to capture the image and one to retract the eyelids. The quality of the scan was poor due to the surface drying out even after instillation of artificial tears and the patient squeezing her lids. However, there was valuable information extrapolated from the scan (Figure 2). The CSP display shows the sagittal height of the patient’s right eye at specific diameters. The different colors displayed suggest that the patient’s sclera is highly irregular and will benefit from a free-form design. The parameters of the diagnostic lens tried on in office, including the back optic zone radius, power, and over-refraction, were provided to the lab with the patient’s refractive data to determine the power of the free-form lens. The CSP revealed that at a 16.8 mm diameter chord, the patient had 1101 microns of toricity, explaining why none of the diagnostic lenses would stay on the right eye. In working with consultation, a free-form or image-guided design was created to correct for the high corneal and 4 quadrants of different scleral toricity. The parameters of the free-form design for the right eye were base curve 7.85, sagittal depth of 4511 microns, power -2.00, overall diameter 16.8 mm, and quadrant specific landing zone (Figure 3). There was no over-refraction, and the patient was immediately impressed by her clarity in vision in her right eye, 20/30. The image-guided scleral lens fit was much improved from the diagnostic lenses. Slit lamp examination of the right eye showed central clearance of approximately 300 microns immediately after application without any corneal touch. There was full limbal clearance 360 degrees of approximately 40-50 microns. The flat scleral landing zone settled at the 12/6 o’clock position.16 Markings for this specific lens design will gravitate to the flatter or more shallow meridian.

There was 360 degrees of ocular alignment of the landing zone, without impingement, compression, or edge lift. These findings were confirmed with anterior segment optical coherence tomography. The patient had excellent initial comfort with the scleral lens on her right eye and greatly appreciated increased clarity compared to her habitual vision. The left eye was fit with a soft toric contact lens which provided vision of 20/20.
The patient completed appropriate application and removal training successfully. The patient was instructed to use preservative free saline to fill the bowl of the scleral lens prior to lens application and hydrogen peroxide solution for nightly disinfection. She was also provided a large DMV® scleral cup™ tool (DMV Corporation, Zanesville, OH) for application, and a small nonvented DMV scleral cup™ for removal. The patient was scheduled for follow-up in 2 weeks and instructed to wear the lenses for 4 hours prior to her appointment.
The patient returned for a follow-up visit 2 weeks later. She reported doing well overall with her scleral lens and was happy with the improved level of vision. She had no issues with application or removal and wore it daily, approximately 12-15 hours per day. Visual acuities were 20/25+ right eye and 20/20 left eye. Pupils, confrontation visual fields, and extraocular motilities were normal. The scleral lens fit was assessed at the slit lamp. She had been wearing the lens for approximately 6 hours that day. The fit with slit lamp examination and anterior segment optical coherence tomography showed a central corneal vault around 260 microns in the right eye which was acceptable as the center thickness of the lens was 300 microns, providing a 1:1 central fitting ratio. There was no limbal touch, with clearance of approximately 30-40 microns. The vertical landing zone (12 and 6 o’clock position) showed slight compression and no associated conjunctival stain or rebound hyperemia after removal. The horizontal landing zone was well aligned without conjunctival stain after removal. All other anterior segment findings were unremarkable. The patient was re-educated on scleral lens care and management and was instructed to return for a follow-up in 3 months.
The patient returned for a 3-month and 6-month follow-up and reported great ocular comfort and vision with her scleral lens. She denied difficulty with lens application or removal and was using the appropriate fill and disinfecting solutions. No corneal, limbal, or conjunctival stain was present with lens removal at either visit. She was instructed to continue wearing her scleral lens and return annually for examinations.
DISCUSSION
Scleral lenses can be a very effective method for treatment and visual rehabilitation for patients.1,3,9 By utilizing a gas permeable material that maintains a uniform shape, SLs offer superior visual acuity and quality of vision compared to conventional correction such as spectacles. The fluid reservoir of SLs optically neutralizes anterior corneal astigmatism and effectively reduces higher order aberrations that may cause visual distortions.2,11 Additionally, with a properly aligned landing zone, SLs ensure significant improvement in visual stability. This patient enjoyed much improved visual clarity and an improved scleral lens fit with an image-guided or free-form scleral lens design. For patients with significant corneal and scleral toricity, SL designed by utilizing profilometry may be an excellent option to provide functional vision and ocular surface support.10,12,13,19
Scleral lens fitting can be rewarding yet challenging for some patients with irregular ocular surfaces. Utilizing profilometry to design image-guided scleral lens designs should provide a more accurate fit along with alignment of the landing zone.10,12,19,20 However, incorporating technology to design customized SL has limitations, particularly if a good quality scan is not achieved. Technology also does not replace the need for skilled clinical evaluation of the SL on the patient’s eye.
Corneoscleral profilometry measurements may be acquired with several instruments. The OCULUS Pentacam® CSP (OCULUS, Inc.) was utilized for this patient’s image-guided scleral lens design. The CSP does not require use of sodium fluorescein to capture an image and allows practitioners to scan the sclera up to 18.0 mm in diameter. This is beneficial for patients with increased scleral toricity and conjunctival irregularities by providing detailed information when fitting large diameter SL.21 The patient’s small palpebral apertures (8.0 mm) made it difficult to obtain a high-quality scan. Two examiners were needed to acquire this patient’s scans, one to capture the image and one to retract the eyelids. When fitting image-guided SL, an over-refraction is performed with a diagnostic lens to provide the lab with the patient’s refractive data.10,22
Scleral toricity has been defined in the literature as the difference in scleral elevation between 2 meridians. As distance from the limbus increases, scleral toricity also increases.10,11 Scleras fit with smaller diameter lenses (<15 mm) may not need customized landing zones as there is less toricity closer to the limbus.23 Corneal astigmatism has a high probability of following scleral astigmatism in astigmatic eyes.16 The steeper meridian of the cornea does not always correlate to the steep meridian of the sclera. However, scleras fit with larger diameter SL (>15 mm) will need toric or customized landing zones due to the increased toricity.11,24 Due to the patient’s scleral toricity, she failed with diagnostic lens fits of small and large diameters. Neither a spherical nor toric landing zone would provide an adequate fit for this patient. The patient had almost 1100 microns of scleral toricity, making the SL fitting with diagnostic lenses challenging. Utilization of corneoscleral profilometry allowed for more precise fitting with an image-guided SL design.
CONCLUSION
Profilometry helps practitioners create customized SL. Profilometry-guided scleral designs may be an option for patients with high corneal and scleral toricity when other options fail. Further study is needed to identify when profilometry should be utilized and how it can be most beneficial in clinical practice.
TAKE HOME POINTS
-
Larger diameter SL will often need more customization to provide alignment with the landing zone.
-
Utilization of corneoscleral profilometry allows for more precise fitting with an image-guided SL design.
-
Profilometry-guided scleral designs may be an option for patients with high corneal and scleral toricity.
Patient Consent
No identifiable health information was included in this case report.
Human Rights
Procedures were followed in accordance of the Helsinki Declaration.
Conflicts of Interest
The authors have no direct conflict of interest with any products discussed in this manuscript. The authors received consultation on lens design via ValleyContax Custom Contact Lenses.
Funding Sources
The authors declare no conflicts of interest.
Data Availability
No data is available for this report.
Artificial Intelligence (AI) use
AI was not used in the creation or submission of this manuscript.