Introduction
Medroxyprogesterone acetate is a synthetic progesterone commonly used around the world as a contraceptive that is injected intramuscularly or subcutaneously.1 Often, medroxyprogesterone acetate is dosed at 150 mg/mL intramuscularly (Depo-Provera®; Pfizer Inc., New York, NY), and is dosed 104 mg/0.65 mL subcutaneously (Depo-SubQ Provera 104®; Pfizer Inc., New York, NY).2 Medroxyprogesterone acetate inhibits gonadotropin-releasing hormones by binding to progesterone receptors located in the hypothalamus, resulting in a downstream response that prevents ovulation, sperm mobility, and follicular maturation.3 Other indications include amenorrhea,4 endometrial hyperplasia prevention,5 and endometrial carcinoma.5
Depo-Provera was approved by the United States Food and Drug Administration for use as contraception in 1992. In 2000, Hensiek et al reported the first case of meningioma development after 4 years of medroxyprogesterone acetate usage.6 Since then, there has been increasing evidence of an association between medroxyprogesterone acetate usage and meningioma growth. In 2024, a large study examining the association between various progestogens and intracranial meningioma reported a 5.6-fold increased risk associated with prolonged use of medroxyprogesterone acetate.7 Meningiomas in the study requiring surgery were most frequently located at the skull base with the majority of those in the anterior cranial fossa, where the anterior visual pathway is located. In this report, we describe a case of visual decline as an initial symptom in a patient with long-term medroxyprogesterone acetate use that led to the discovery of an anterior clinoidal meningioma.
Case Report
A 55-year-old Black woman presented to clinic with complaints of progressive vision loss in her right eye over the past 6 months. She denied any associated eye pain or diplopia. Her ocular history was remarkable for cataracts. Her medical history was remarkable for migraines, hypothyroidism secondary to thyroidectomy 8 years ago, and seizure disorders. Current medications included levetiracetam, levothyroxine, and history of depot medroxyprogesterone acetate (Depo-Provera) use for greater than 5 years. Notably, a previous magnetic resonance image performed 8 years ago had been unremarkable.
Best-corrected visual acuity measured 20/150 in the right eye and 20/25 in the left eye. Pupillary examination revealed pupils that were equal, round, and reactive to light in both eyes, with a 1.8 log unit relative afferent pupillary defect in the right eye.
Confrontation visual field testing showed a large central relative scotoma in the right eye with full peripheral responses while the left eye was full to finger counting. Extraocular motilities were full in the right and left eye without pain or double vision. Color vision testing using Ishihara plates demonstrated 0/14 correct (unable to see test plate) in the right eye and 14/14 in the left eye. Exophthalmometry measurements were 19 mm in the right eye and 18 mm in the left eye with a base of 99 mm . Intraocular pressures measured with iCare® were 8 mm Hg in the right eye and 9 mm Hg in the left eye. Blood pressure was 122/80 mm Hg.
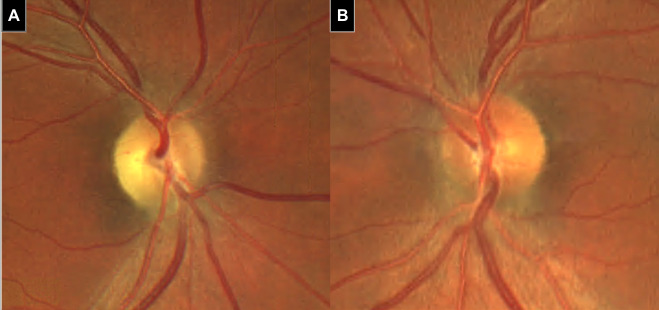
Dilated fundus examination revealed small optic discs bilaterally. The right optic disc showed 1+ diffuse pallor with 2+ temporal pallor and a cup-to-disc ratio of 0.25 (Figure 1). The left optic disc also had a 0.25 cup-to-disc ratio with no definite pallor. The retina was unremarkable in both eyes.
_and_left_(b)_eye_s_optic_disc._the_right_eye_has_1__di.png)
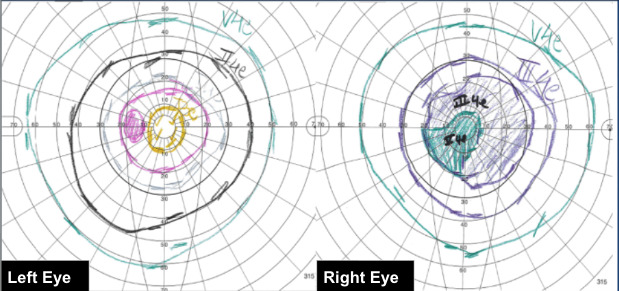
Figure 2 shows Goldmann visual field testing which demonstrated a central defect in the right eye extending 20 degrees superiorly, inferiorly, and nasally, and 30 degrees temporally with the III4e isopter. The left eye exhibited a full visual field.

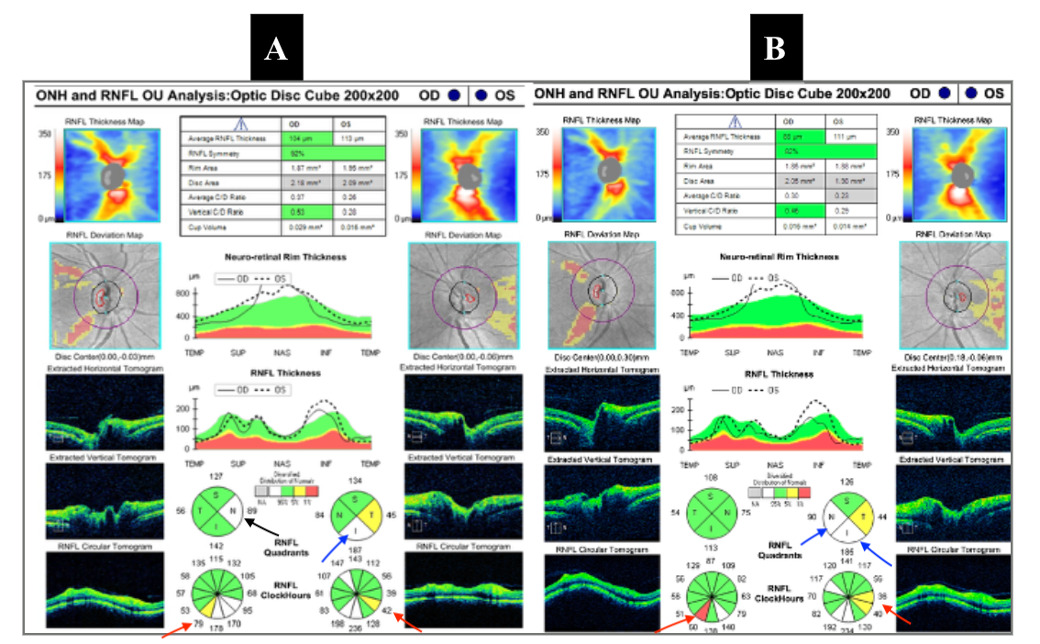
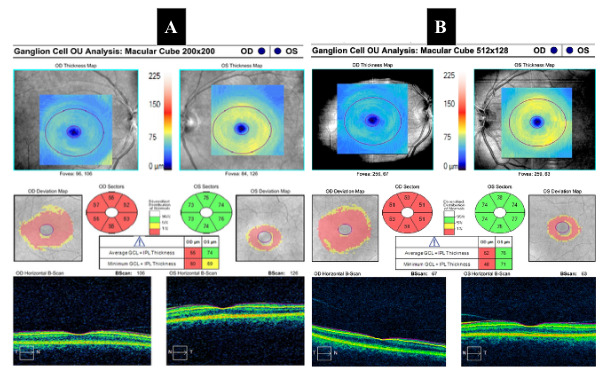
Figure 3 shows optical coherence tomography of the optic nerve which revealed small optic discs bilaterally. The right eye showed nasal retinal nerve fiber layer elevation while the left eye demonstrated inferior retinal nerve fiber layer elevation. Vitreopapillary traction was present in both eyes. Figure 4 shows optical coherence tomography of the macula and ganglion cell complex which showed diffuse thinning 360 degrees in the right eye while the left eye was within normal limits.
_presurgical_optical_coherence_tomography_of_optic_nerve_of_both_eyes__showing_elevated.png)
_presurgical_optical_coherence_tomography_of_macula_(right)_showing_diffuse_thinning_in.png)
A comprehensive laboratory work-up for possible causes of nonglaucomatous optic neuropathy was ordered, including complete blood count with differential, platelet count, erythrocyte sedimentation rate, C-reactive protein, serum folate, vitamin B12, Lyme titer, rapid plasma reagin, fluorescent treponemal antibody absorption, angiotensin-converting enzyme, antinuclear antibody with reflex, methylmalonic acid, and serum protein electrophoresis. At the time of this visit, she had already been scheduled for a brain magnetic resonance imaging with and without contrast by her neurologist due to history of migraines and the known risk of meningioma associated with long-term medroxyprogesterone use. We were unable to add an orbital study at the time and decided to wait for the brain magnetic resonance imaging results before ordering a dedicated orbital study.
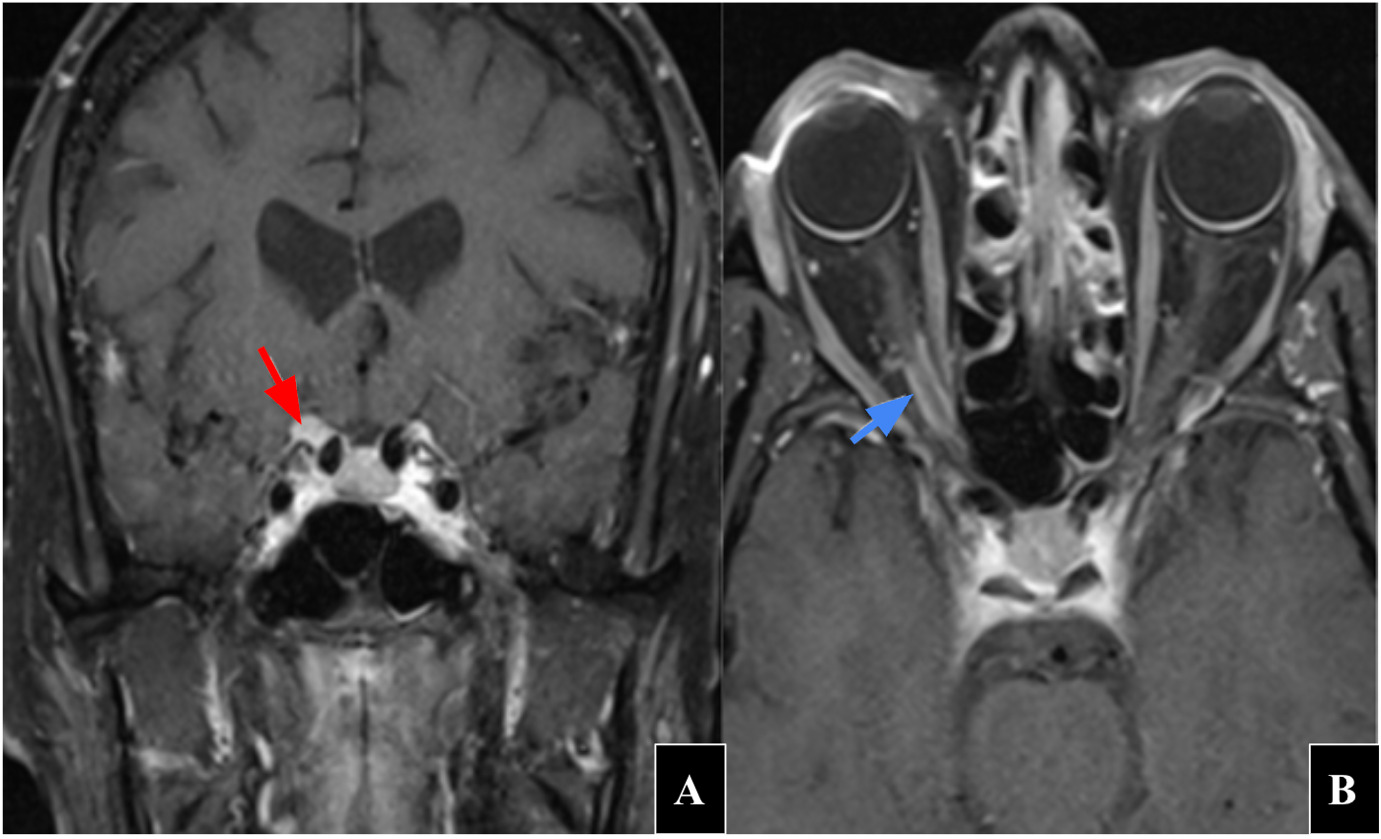
Her laboratory workup was unremarkable for any inflammatory or infectious etiologies. Her brain magnetic resonance image with and without contrast revealed scattered nonspecific punctate and patchy foci of T2 hyperintense signal without mass effect in the bilateral subcortical and periventricular white matter and corona radiata, likely due to minimal chronic microvascular ischemic changes. The report also stated T2 hyperintense signal present in the cortex of the posterior left frontal lobe with associated volume loss likely reflecting small chronic infarction. An exact etiology for her vision loss in the right eye was not noted on the magnetic resonance image brain report. However, upon review of the images and discussion with the radiologist, it was determined that there was some increased T2 signal around the right optic nerve. A dedicated orbital magnetic resonance image with and without contrast was ordered. The orbital magnetic resonance image revealed a 9 × 11 × 5 mm type III anterior clinoidal meningioma extending into the optic canal along the optic nerve sheath (Figure 5). Based on these findings, she was scheduled to see a neurosurgeon and underwent a right fronto-orbital craniotomy with tumor resection which was completed without complications. She also discontinued medroxyprogesterone therapy.
_contrast-enhanced_coronal_t1_magnetic_resonance_imaging_showing_9_x_11_x_5_millimeter_.png)
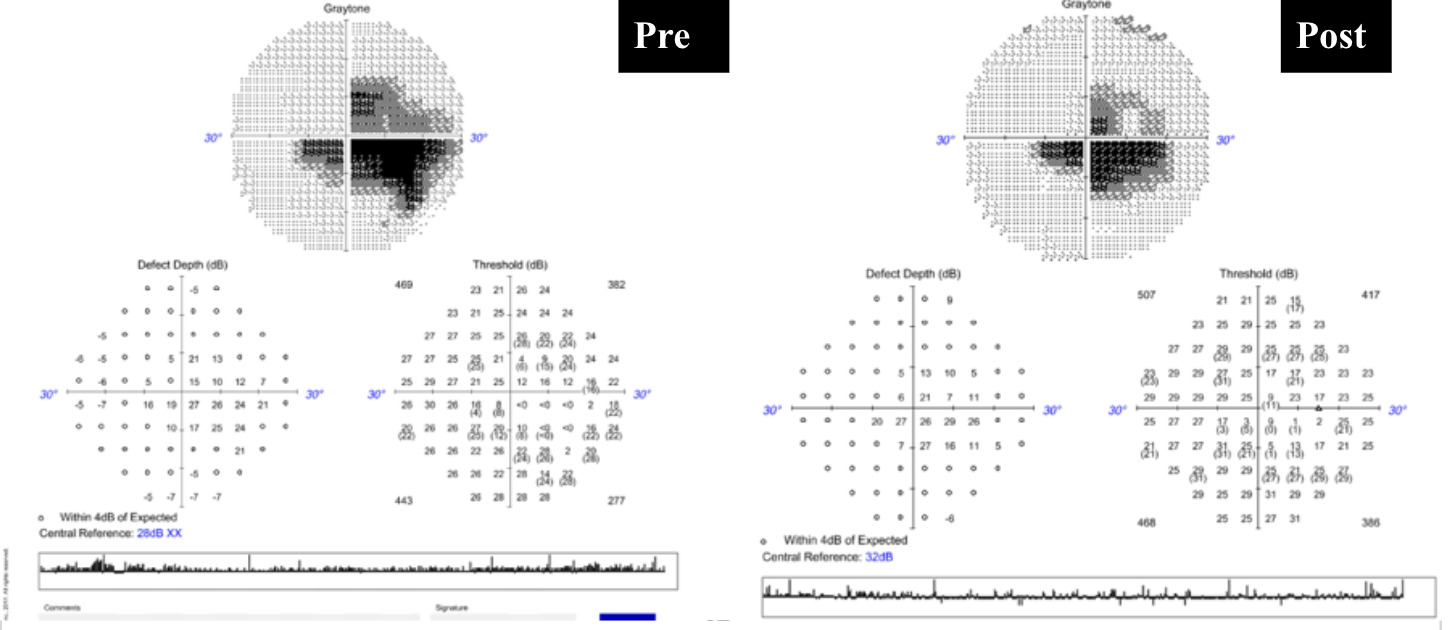
At her initial follow-up, 1-month postoperative, visual acuity had improved to 20/60 in the right eye and remained 20/25 in the left eye. Pupillary testing showed that her pupils were equal, round, and reactive to light in both eyes with a 1.5 log unit relative afferent pupillary defect persisting in the right eye. Postoperative optical coherence tomography of the retinal nerve fiber layer demonstrated thin retinal nerve fiber layer inferior in the right eye and borderline thin temporal in the left eye with elevated areas nasal and inferior in the left eye as shown by figure 3. The ganglion cell complex was stable to initial visit as shown by figure 4. Comparison of presurgical (left) and postsurgical (right) visual field testing revealed slight improvement with persistent central scotoma but preserved peripheral vision in the right eye as shown by figure 6.
_to_1_month_postsurgical_vi.png)
At 3-month postoperative follow-up, visual acuity continued to improve to 20/40 in the right eye. Her visual field continued to show a stable large central scotoma in the left eye. Her left eye remains intact.
These findings were consistent with partial optic nerve recovery following decompression. Prognosis for further visual recovery is guarded due to evidence of preexisting axonal loss on optical coherence tomography and ganglion cell complex analysis.
Discussion
Anterior clinoidal meningiomas are benign tumors that arise from meningothelial cells localized at the anterior clinoid process of the lesser sphenoid wing. Anterior clinoidal meningiomas are categorized into 4 major types, each defined by its origination in the anterior clinoid process: type I, arising from the superior surface of the anterior clinoid process; type II, arising from the lateral surface (IIa) or the tip of the anterior clinoid process (IIb); type III, arising from the medial surface of the anterior clinoid process; and type IV, in which the site of origin cannot be clearly determined.8 Each type of these anterior clinoidal meningiomas frequently causes vision loss due to its proximity to the anterior visual pathway, specifically the optic canal which is the region where the optic nerve and ophthalmic artery traverse. Giammetti et. al indicated that 66% of patients with anterior clinoidal meningiomas presented with vision impairment.9 Signs and symptoms which may indicate an anterior skull base lesion include proptosis (due to extension into the orbital cavity), optic nerve head pallor, peripheral visual decline, and visual disturbances.9,10 Clinical findings that are suggestive of a compressive optic nerve lesion should always warrant an orbital magnetic resonance imaging study with and without contrast.11 In this case, our patient came in presenting with optic atrophy and central visual decline along with an afferent pupillary defect in her right eye. The magnetic resonance imaging report was consistent with her ocular findings as type III anterior clinoidal meningiomas extend medially from the anterior clinoid process toward the optic nerve.12
Most meningiomas express progesterone receptors.13 This is the likely reason why the incidence of meningioma growth has long been observed to occur more frequently in premenopausal women. A higher expression of progesterone receptors was observed in premenopausal women (78.2%) compared with men (65.1%) and postmenopausal women (68.4%).14 Previous studies also demonstrated an increased association between meningioma development and exposure to certain progestogen therapies, including cyproterone acetate, nomegestrol acetate, and chlormadinone acetate.7,15 More recently, a large study published in 2024 identified the strong association between meningioma growth and the use of medroxyprogesterone acetate, medrogestone, and progestone.3
Although research is still ongoing and the exact pathophysiology is poorly understood, accumulating evidence supports an association between meningioma growth and exposure to certain progesterone therapies.16 This highlights the importance of monitoring patients who are undergoing progesterone therapy for neurological changes and, especially, ocular changes since progesterone associated meningioma tend to have a greater localization at the anterior and middle fossa of the skull making the anterior visual pathway susceptible to compressive neuropathy.15,17 Although there is no standardization on the frequency of radiological imaging in patients taking progesterone therapy, orbital magnetic resonance imaging study with and without contrast should always be ordered when clinical findings suggestive of compressive etiologies present, especially when on hormonal therapy. Additionally, a baseline preventive orbital magnetic resonance imaging study should be considered prior to initiating hormonal therapy, particularly in patients with risk factors such as a family history of meningioma, prior exposure to ionizing radiation, or genetic disorders.18
There is an increased risk of meningioma in patients with known genetic markers, such as the NF2 gene. In this population, the risk may be amplified by progesterone therapy. If these genetic disorders are clinically suspected, genetic testing should be considered. Otherwise, prior genetic testing will likely cause unnecessary emotion burden, care disruption, and cost.7,19
Meningioma regression has been reported following discontinuation of progesterone therapy.20 The main indication for surgical intervention is cranial neuropathies from tumor compression.21 Since our patient’s visual field testing demonstrated significant central vision loss along with significant loss on ganglion cell complex analysis, surgical intervention was warranted. Due to their close relationship in blood supply and proximity to the optic nerve, anterior clinoidal meningiomas are associated with poorer function outcomes and higher rate of subtotal resections compared to other meningioma resections in the anterior skull base. In a case series of 10 patients, Alam et al reported favorable surgical outcomes in patients with anterior clinoidal meningiomas with 70% demonstrating significant postoperative surgical visual improvements.22 In contrast, a more recent meta-analysis by Giammattei et al evaluating surgical outcomes for clinoidal meningiomas reported less favorable visual outcomes with fewer than 50% of patients exhibiting postoperative improvement in visual acuity.9 Furthermore, Giammattei et al noted a rate of 20.9% of optic canal invasion in cases with anterior clinoidal meningioma. Our patient underwent a fronto-orbital zygomatic craniotomy to reduce the likelihood of further progression of the meningioma invasion and possibly improve her symptoms. Although there is a poor visual improvement outcome with major complications after surgery for anterior clinoidal meningiomas, her postoperative visual acuity outcome did demonstrate significant improvement from 20/200 to 20/40 in her right eye without any significant surgical complications.
Conclusion
We present a rare case of an anterior clinoidal meningioma presumably due to long term medroxyprogesterone usage resulting in visual decline. Recognition of the patient’s medication history is crucial to diagnosis, management, and treatment plan as certain hormonal drugs can contribute to development of compressive lesions, such as meningioma, with significant visual consequences. Therefore, patients on certain types of progesterone therapy should be closely monitored with regular ocular examinations to allow for early detection of visual or other neurological changes. This will increase the likelihood of prompt neuroimaging and timely intervention, thereby optimizing visual prognosis.
Take Home Points
-
Early recognition of medication history such as hormone-associated risk factors can directly influence clinical decision making such as imaging of the head and neck.
-
Long-term medroxyprogesterone acetate use may be associated with meningioma development which can cause compressive optic neuropathies and/or other neuropathies, warranting magnetic resonance imaging studies if suspected.
-
Frequent monitoring of ophthalmic and neurological status is warranted in patients receiving hormones associated with meningioma growth.
Patient Consent
Written and verbal patient consent was not obtained for this case report. This case report does not contain any identifying health information.
Human Rights
Human participants in this case study follows in accordance with the ethical standards of the Helsinki Declaration. Ethics approval was not obtained nor required for this study as it falls in accordance with guidelines.
Conflict of Interest
The authors have no conflicts of interest to declare.
Funding Sources
This study was not supported by any sponsor or funder.
Data Availability
The data that support the findings of this study are available on request from the corresponding author, ED. The data are not publicly available due to personal identifying information.
Artificial Intelligence (AI) Use
Artificial intelligence (AI) technologies were not used in the preparation of this manuscript.