
INTRODUCTION
Lens-induced glaucoma is a secondary glaucoma that can present as either angle-closure or open-angle glaucoma.1 Secondary angle-closure glaucoma occurs when an intumescent lens displaces forward, inducing pupillary block and causing iris bombé and iridotrabecular contact. This mechanism obstructs aqueous outflow through the trabecular meshwork, leading to an acute rise in intraocular pressure.2,3 Secondary open-angle glaucoma arises from lens proteins and inflammatory cells blocking the trabecular meshwork and impeding the outflow of aqueous humor, also resulting in an acute rise in intraocular pressure.4 Phacolytic glaucoma is a form of the latter and is associated with soluble lens protein leaking into the anterior chamber through microperforations in a hypermature cataract with an otherwise intact capsule.1,3
Improved cataract outreach programs combined with advancements in cataract surgical procedures have made hypermature cataracts and their complications increasingly uncommon. However, although phacolytic glaucoma is a rare complication, it can still present in patients who have a neglected cataract due to a number of reasons, including poor access to health care. Delayed diagnosis and treatment in these patients usually results in poor visual outcomes. Poor visual prognosis is associated with secondary complications, including corneal decompensation, elevated intraocular pressure that is refractory to medical management, and the development of glaucomatous optic atrophy.5 Therefore, it is essential that eyecare providers are able to identify phacolytic glaucoma and initiate the appropriate treatment and referral process for these patients.
This case report describes a patient who developed phacolytic glaucoma due to a neglected hypermature cataract. The clinical presentation, differential diagnoses, and treatment and management are discussed. Prompt diagnosis and management are crucial in ensuring patients have the best visual prognosis and mitigating secondary complications. No identifiable health information was included in this case report.
CASE REPORT
A 72-year-old African American man presented complaining of a painful red right eye that began 8 days prior. He reported a history of being hit with a rock in the right eye at age 13 years, which resulted in longstanding decreased vision. However, the patient reported that he felt his vision in the right eye had further worsened since the onset of his recent symptoms. His medical history was positive for hypertension and hypercholesterolemia, for which he was taking amlodipine and atorvastatin, respectively. The patient had no known drug allergies.
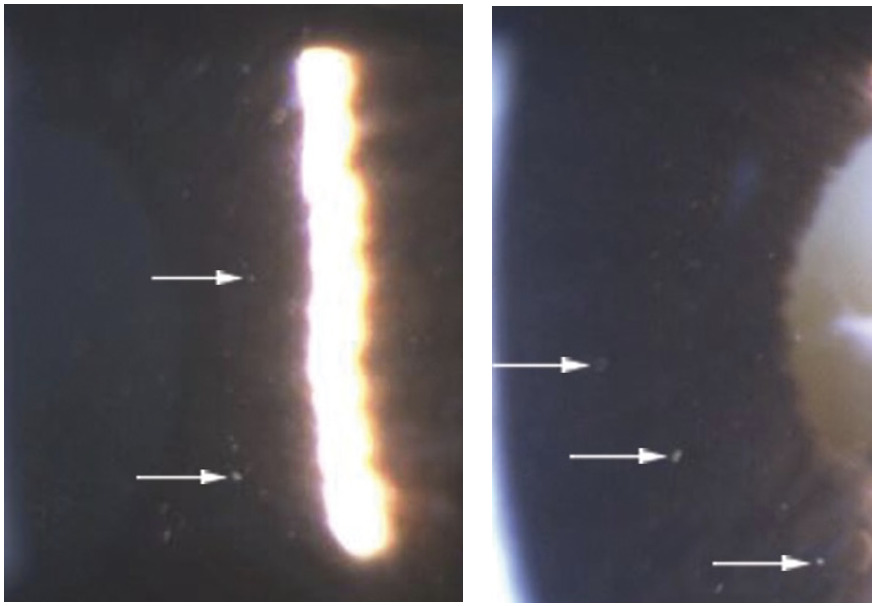
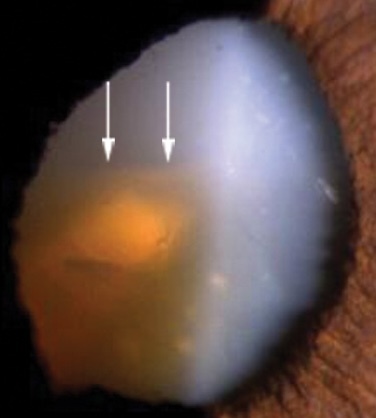
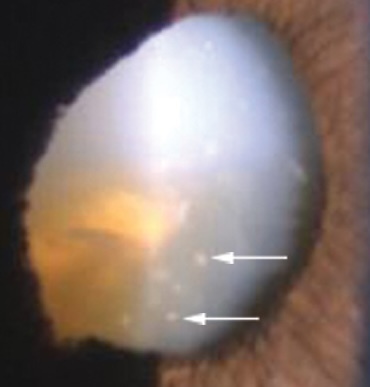
The patient’s uncorrected distance visual acuity was light perception with projection in the right eye and 20/30 in the left eye, with the left eye improving to 20/25 with pinhole. Pupils were round and reactive in both eyes; however, the right pupil showed a more sluggish response to light compared with the left eye, and an afferent pupillary defect was detected in the right eye. Confrontation visual fields could not be tested in the right eye because of the decreased vision but were full to finger counting in the left eye. Extraocular muscle testing showed full range of motion in both eyes. On anterior segment evaluation of the right eye, there was 2+ diffuse injection of the bulbar conjunctiva, 2+ microcystic corneal edema, and diffuse iris atrophy with a peaked pupil. Evaluation of the anterior chamber revealed a deep chamber with the presence of 1+ flare, 2+ cells, which were large and translucent in appearance (Figure 1), as well as white flocculent material floating within the anterior chamber (Figure 2). Examination of the right lens revealed a hypermature cataract with a sunken sclerotic nucleus (Figure 3), the distinct presence of large cells on the anterior lens capsule (Figure 4), and phacodonesis. Anterior segment findings for the left eye were within normal limits, apart from an immature nuclear sclerotic cataract. Van Herick angles were measured to be 4+ nasally and temporally in both eyes. Intraocular pressure measured with Goldmann applanation tonometry was 44 mm Hg in the right eye and 12 mm Hg in the left eye.




Immediate intraocular pressure–lowering treatment was initiated for the right eye. One drop of both apraclonidine 0.5% and brimonidine tartrate 0.2%-timolol maleate 0.5% (Combigan; AbbVie)) was instilled in the patient’s right eye, 15 minutes apart. Additionally, the patient was given two 250 mg acetazolamide tablets to take by mouth. The intraocular pressure was successfully lowered to 15 mm Hg in the right eye within 2.5 hours of initiating treatment. Gonioscopy was then performed to more thoroughly evaluate the angle: the angle was open to ciliary body in both eyes, although angle recession was noted in the right eye superiorly and superonasally, presumably secondary to the patient’s previous history of ocular trauma. Because of the hypermature cataract and no view of the posterior segment with undilated fundus examination of the right eye, brightness scan ultrasonography was obtained. The results confirmed an intact retina with a moderate amount of vitreal debris. Undilated fundus examination of the left eye showed a healthy, well-perfused optic nerve head that was flat with distinct margins. The cup-to-disc ratio was graded as 0.5 round. The macula and vessels appeared normal to the extent viewed.
Differential diagnoses that could be considered with the patient’s history of ocular trauma, elevated intraocular pressure, and lens appearance include angle recession glaucoma and lens-induced glaucomas, such as phacomorphic glaucoma, phacolytic glaucoma, lens-particle glaucoma, and phacoantigenic glaucoma. Angle recession glaucoma is a secondary open-angle glaucoma that should be considered in patients with a history of ocular trauma and unilateral elevated intraocular pressure. Ocular trauma may cause a tear between the circular and longitudinal fibers of the ciliary body, resulting in angle recession and a chronic rise in intraocular pressure, even years after the initial injury.6 Although angle recession glaucoma was considered given the patient’s history of ocular trauma and the confirmed angle recession on gonioscopy, it was ruled out because of the acute onset of pain and decreased vision, markedly elevated intraocular pressure, and inflammatory reaction in the presence of a hypermature cataract. Phacomorphic glaucoma is a secondary angle-closure glaucoma that occurs as a result of pupillary block by an intumescent lens.1 Although the patient had a hypermature cataract, the presence of a deep anterior chamber and open angles immediately excluded phacomorphic glaucoma. Phacolytic, lens-particle, and phacoantigenic glaucoma are lens-induced secondary angle-open glaucomas. Phacolytic glaucoma occurs in the setting of a hypermature cataract when soluble lens proteins leak into the anterior chamber through microperforations in an otherwise intact lens capsule.1,5 This elicits an immune response in the eye, leading to macrophages depositing on the lens surface. The lens proteins and macrophages become entrapped within the trabecular meshwork, resulting in decreased outflow and increased intraocular pressure.7 Phacolytic glaucoma should strongly be considered as a differential in cases of elevated intraocular pressure in the presence of anterior chamber inflammation and a hypermature cataract.1 Patients will typically present with an acute-onset, painful red eye and significantly decreased vision, as was seen in this patient.3,4 In lens-particle glaucoma, patients will present with signs and symptoms similar to phacolytic glaucoma. However, unlike phacolytic glaucoma, in this case, a disrupted lens capsule allows for lens fragments to enter the aqueous humor.1,8 Lens-particle glaucoma typically occurs after penetrating lens trauma or cataract surgery, as spontaneous rupture of a hypermature cataract is rare.1,9 It characteristically presents within a few weeks of the inciting event, although cases occurring months to years later have been reported.9–11 Phacoantigenic glaucoma occurs when there is lens capsule rupture, either secondary to trauma or ocular surgery, with the inciting event occurring 1 to 14 days before the onset of inflammation. It is a granulomatous inflammatory condition; thus, it typically presents with mutton-fat keratic precipitates and posterior synechiae.12 Because of the absence of recent ocular trauma, lack of lens fragments within the anterior chamber, no signs of granulomatous inflammation, and the presence of an intact lens capsule, lens-particle and phacoantigenic glaucoma were ruled out.
Based on the patient’s history and clinical signs and symptoms, he was diagnosed with phacolytic glaucoma. Ophthalmology was consulted, and the patient was seen the following day. The patient was educated on the immediate need to keep intraocular pressure low and reduce inflammation in the eye. He was prescribed brimonidine tartrate 0.2%-timolol maleate 0.5% to use twice daily and prednisolone acetate 1% to use 4 times daily in the right eye.
At the consultation with ophthalmology, the patient’s intraocular pressure remained stable, treatment was kept the same, and cataract surgery was scheduled for 6 days later. Because of the hypermature cataract and presence of phacodonesis, indicating weak zonular support of the lens, the patient underwent an extracapsular technique that did not use phacoemulsification. The patient was fitted with a 3-piece intraocular lens in the ciliary sulcus because of the lack of zonular support.
At the 2-week postoperative appointment, vision improved from light perception with projection to count fingers at 2 feet in the right eye. The patient confirmed a subjective improvement in vision and denied eye pain. The intraocular pressure remained stable at 18 mm Hg without pressure-lowering medications in the right eye, whereas the intraocular pressure in the left eye was 14 mm Hg. The asymmetric intraocular pressures and angle recession noted on gonioscopy warranted continued monitoring for the development of angle recession glaucoma in the right eye. Dilated fundus examination findings for the right eye revealed significant myopic degeneration with presumed nonglaucomatous myopic optic nerve atrophy, which made it difficult to accurately assess and grade the cup-to-disc ratio. Additional findings included a posterior staphyloma and diffuse chorioretinal scarring. These findings correlated with asymmetric axial lengths of 30 mm in the right eye and 25 mm in the left eye measured prior to the patient’s cataract surgery and likely explained the patient’s limited visual prognosis and presence of afferent pupillary defect in the right eye. The patient will continue to be monitored regularly in an outpatient setting.
DISCUSSION
Phacolytic glaucoma is a rare form of acute secondary open-angle glaucoma that results from the leakage of soluble lens proteins into the anterior chamber through microperforations in an otherwise intact lens capsule.1,5 This pathological process occurs in a hypermature cataract (differentiated from immature or mature cataracts by a higher concentration of high molecular weight proteins), in which phacolysis leads to the rapid liquefication of the lens cortex, and the lens capsule and epithelium undergo degenerative changes, resulting in a more permeable lens capsule.7,13 Phacolysis is driven by two enzymes, protease A and protease B, which degrade large lens protein molecules into smaller molecules that are then able to diffuse through the hyperpermeable lens capsule.7 The lens nucleus, typically resistant to this degenerative process and surrounded by liquified cortex, can dislocate and sink inferiorly into the capsular bag.14 The abnormal presence of circulating cortical lens proteins within the aqueous humor elicits an immune response within the eye, resulting in large mononuclear phagocytes, specifically macrophages, depositing over the lens surface.7 As they engulf liquified lens cortex material, these macrophages will take on a distinct translucent and larger appearance, which helps differentiate them from other leukocytes, commonly referred to as white blood cells.1,7
Carried by the normal aqueous flow, lens proteins and macrophages become entrapped within the trabecular meshwork filtration tissue, resulting in decreased aqueous outflow and increased intraocular pressure.7 Previously, it was assumed that the engorged macrophages are the primary obstruction of the trabecular meshwork in phacolytic glaucoma. However, morphologic examination of anterior chamber fluid in these patients has shown that it is actually the accumulation of high molecular weight soluble lens proteins (absent in infant and young adult lenses but increasing in concentration from ages 20 to 60 years) that causes mechanical obstruction of the trabecular meshwork.1,15 Additionally, no other cells are present in significant concentrations.7
Anterior chamber fluid analysis has also shown that the fluid lacks fibrinogen, which explains the absence of synechiae formation in patients with phacolytic glaucoma.7 Fibrinogen is a precursor of fibrin, which plays an essential role in inflammatory adhesions.16 The importance of fibrin in synechiae formation is further supported in studies demonstrating that postoperative anterior chamber fibrin deposition in eyes that underwent phacovitrectomy was a significant risk factor for subsequent posterior synechiae formation.17 Of note, the macrophages are not inherently sticky, and therefore, they do not commonly aggregate or form keratic precipitates. The absence of synechiae and keratic precipitates helps differentiate phacolytic glaucoma from other inflammatory conditions.7
Patients with phacolytic glaucoma symptomatically present with an acute onset of a painful injected eye and significantly decreased vision, often reduced to hand motion or worse.3,4 Given that this condition occurs as a result of a hypermature cataract, in which there is already a gradual and significant decline in vision over time, the patient’s subjective complaints of acute vision loss may vary.7 Notably, in most cases, the patient’s fellow eye has good vision.7 Ayub and colleagues conducted one of the largest studies on patients with lens-induced glaucoma, the majority of which were phacolytic.15 They reported that good vision in the contralateral eye was the primary reason for deferred cataract surgery. In most cases, the fellow eye was either pseudophakic (72%) or had an immature cataract, demonstrating how good vision in one eye can lead to delayed treatment of a hypermature cataract in the fellow eye.18
Clinical findings of elevated intraocular pressure with open angles on gonioscopy, in the presence of a hypermature cataract, should prompt careful evaluation of the patient’s anterior chamber.1 Anterior chamber evaluation will reveal flare and macrophages, which are larger and have a more translucent appearance than white blood cells seen in uveitis.1,19 White flocculent material, presumed to be liquified lens cortex, and refractile particles, identified as cholesterol crystals, may also be seen in the anterior chamber.7,20,21 These cholesterol crystals are thought to originate from degraded lenticular cell membrane.22 Collection of lens protein material and crystals layered in the inferior anterior chamber may form a pseudohypopyon.23,24 Patients can also present with corneal edema as a result of markedly elevated intraocular pressure.7
The definitive treatment for phacolytic glaucoma is cataract extraction.1,25,26 However, the initial management includes promptly lowering intraocular pressure and reducing inflammation, which is essential in reducing the risk of permanent vision loss and intraoperative complications.5 Topical steroids are effective in reducing inflammation and may initially help lower intraocular pressure; however, these effects are generally temporary.1 Sustained intraocular pressure reduction can be achieved through the use of aqueous suppressants, including oral or topical carbonic anhydrase inhibitors, topical alpha-2 agonists, and topical beta-blockers.27 Historically, topical prostaglandin analogues have been thought to exacerbate intraocular inflammation and, therefore, have been considered contraindicated in cases of active inflammation; however, recent literature has challenged that assumption.28 Additionally, cycloplegics should be used with caution when there is a question of lens instability, such as the phacodonesis observed in our patient, as their use can aggravate the condition.29 Prompt cataract extraction typically results in good visual prognosis and favorable intraocular pressure outcomes, assuming the absence of concurrent ocular comorbidities.25,26 In patients presenting within 2 weeks of developing acute symptoms, cataract extraction alone is typically the definitive treatment, and additional glaucoma interventions, such as filtration surgery or continued medical treatment, are rarely necessary.18,30
CONCLUSION
Phacolytic glaucoma is precipitated by the leakage of soluble lens proteins from a hypermature cataract. Given that the leakage of lens proteins and lens-induced inflammation can produce significant ocular signs and symptoms, including pain, markedly elevated intraocular pressure, and vision loss, phacolytic glaucoma should be considered in the differential diagnosis of acute secondary glaucoma with a hypermature cataract. In summary, this case highlights the important role that eyecare providers play in the early recognition and timely management of phacolytic glaucoma, helping to optimize the prognosis for these patients.
DISCLOSURES
- No identifiable health information was included in this case report.
Conflicts of Interest
The author declares no conflicts of interest.
Disclosure of Funding
The author declares no funding sources.