Introduction
Amblyopia is defined clinically as a unilateral or bilateral visual developmental disorder characterized by reduced best-corrected visual acuity in the absence of structural anomalies or ocular disease and attributable to 1 or more amblyogenic factors.1 However, in clinical practice, amblyopia can occur concurrently with ocular disease. In such cases, it has been shown that amblyopia therapy can improve the visual acuity of the affected eye, even though complete improvement may be limited due to the underlying ocular disease.2,3 This article presents clinical cases that add impetus to the preceding clinical insight by demonstrating the efficacy of amblyopia treatment in cases with amblyopia and coexistent foveal hypoplasia.
Foveal hypoplasia is a generic term that describes a retinal disorder characterized by the incomplete development of the fovea. The advent of high-resolution optical coherence tomography imaging has aided immensely in the visualization of the morphological characteristics endemic to foveal hypoplasia. This has enabled the development of a morphology-based grading scale of foveal hypoplasia. Clinically, foveal hypoplasia is graded on a 1-4 scale, with atypical presentation as a separate option.4 These grades are associated with decreasing definition of a foveal pit and lessening extrusion of foveal layers from the plexiform to outer layers of the retina as the grade number increases.4 Best-corrected visual acuity decreases proportionally to the severity of the foveal hypoplasia grade, with grade 1 generally associated with a median acuity range of 0.2 to 0.34 logMAR (20/30 to 20/40 Snellen equivalent) and grade 4 associated with a median acuity range of 0.78 to 0.8 logMAR (20/125 Snellen equivalent).4,5 In clinical practice, mild presentations can be difficult to appreciate in a fundus evaluation alone. Optical coherence tomography can assist in visualizing foveal hypoplasia and evaluating its impact on visual prognosis.
Foveal hypoplasia can coexist with several ocular and syndromic disorders5,6; however, it can occur in up to 3% of clinically normal children7,8 and can also coexist with amblyogenic factors such as strabismus and/or high refractive errors. The latter conditions pose a prognostic challenge especially when determining the independent contributions of amblyopia and foveal hypoplasia to the overall acuity reduction. These prognostic challenges are further exacerbated by the coexistence of nystagmus, which can independently cause an acuity reduction depending on the type and velocity of nystagmus.9 This case series aims to describe foveal hypoplasia as a confounding factor in the diagnosis of amblyopia in 3 pediatric patients. Treatment options are included for 2 cases, in which vision and fusion were improved, and the third case demonstrates the role of electrodiagnostic testing in helping to determine an expected visual acuity endpoint.
Case 1
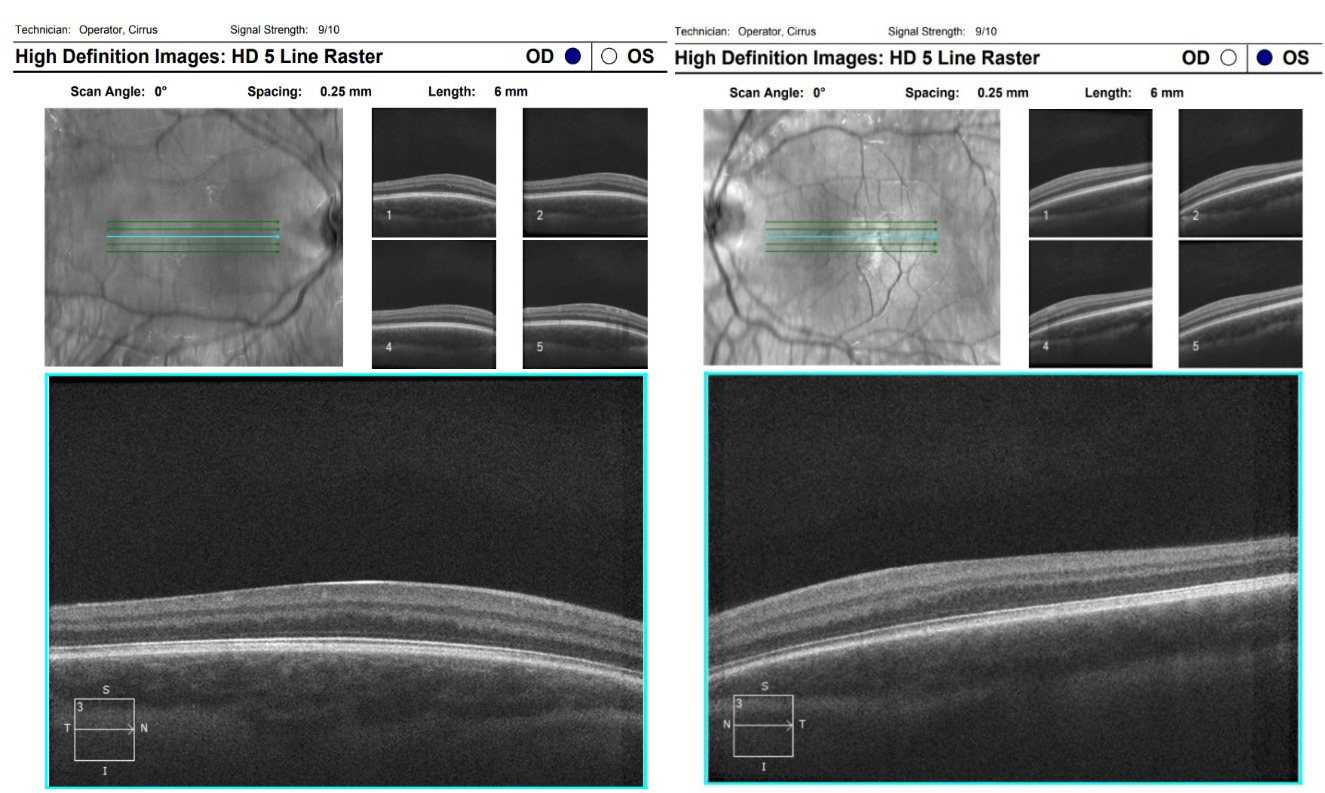
A 14-year-old male patient presented for a comprehensive visual assessment to determine driving eligibility. He had been informed previously that he had reduced vision but could not recall if he had a formal diagnosis of amblyopia when questioned. He reported a positive ocular history for nystagmus, which had been present since birth, and noted current headaches in his review of systems. Personal health history was otherwise unremarkable. He reported full-time spectacle wear for several years, without prior history of patching, atropine, or vision therapy. The habitual spectacle prescription was +3.00 -5.25 x 175 and +1.75 -3.25 x 006, with entering and best-corrected visual acuities of 20/70 and 20/60- in the right and left eyes, respectively, with single letters surrounded by crowding bars and a frosted lens over the contralateral eye. Cover test revealed a high magnitude, nearly constant alternating exotropia. Although extraocular muscles had a full range of motion, he had a horizontal jerk nystagmus, with exacerbation of amplitude in left gaze and dampening in right gaze. There was a latent component to the nystagmus, which was worse in the right eye. Near point of convergence was attempted but unmeasurable, and there was no measurable contour or random dot stereopsis as tested by the stereo fly, Randot Butterfly, or Wirt Rings. Further fusion findings, including Worth Dot, are listed in Table 1. External ocular health was unremarkable, with no transillumination defects of the iris, but the patient had light blonde hair, fair skin, and blue irises. A dilated posterior segment evaluation showed a blonde fundus with no foveal reflex, and a 5-line raster optical coherence tomography scan confirmed grade 3 foveal hypoplasia in both eyes (see Figure 1).

His final prescription based on the cycloplegic refraction at this visit was the same as his habitual prescription, which confirmed amblyogenic astigmatism and anisometropia. Given the lack of prior treatment for his reduced vision and his goal of obtaining a driver’s license, treatment options to potentially improve visual acuity were discussed, although prognosis was guarded given the structural abnormalities of the fovea. Patching was contraindicated because of the latent nystagmus. Management included a referral for fitting of rigid gas-permeable contact lenses to possibly improve the stability of eye movements and potentially visual acuity. Additionally, vision therapy was recommended to improve peripheral fusion and convergence abilities and to decrease the frequency of the exotropia. As many cases of congenital nystagmus exhibit dampening with convergence, the authors were hopeful that improving the patient’s convergence abilities would decrease the nystagmus and increase stability of vision. Both electrodiagnostic and genetic testing for ocular albinism were recommended, but the patient and parent declined these options.
The patient started vision therapy and, prior to completing the program, was successfully fit with rigid gas-permeable contact lenses. Vision therapy sessions emphasized oculomotor and accommodative tasks early in the treatment regimen, with the use of a 20/200 Bangerter foil during monocular activities to reduce latent nystagmus. Following 28 in-office vision therapy sessions, his visual acuity was 20/60 in his right eye and 20/40+ in his left eye through rigid gas-permeable contact lenses, which allowed him to obtain a restricted driver’s license (in Michigan, a restricted license may be issued for individuals with visual acuity of 20/50 to 20/70, with no expected progression of vision loss). A comparison of the prevision and postvision therapy findings, including improvements in fusion and stereopsis, and a list of specific activities are shown in Table 1.
Case 2
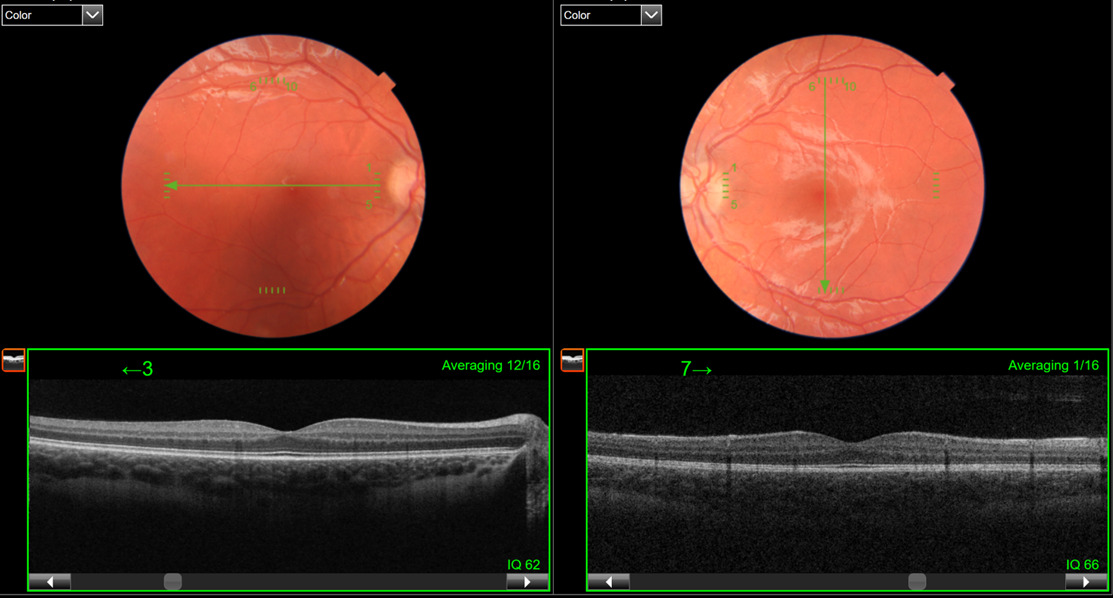
A 9-year-old boy was referred by an eyecare provider for the evaluation and treatment of anisometropic amblyopia. He had been wearing glasses for at least 3 years, and a previous magnetic resonance imaging and other medical history were unremarkable. The patient’s best-corrected visual acuity through +3.00 -0.75 x 165 in the right eye and +4.00 -0.75 x 170 in the left eye was 20/40 and 20/60-, respectively, measured with single letters and crowding bars. The preceding prescription was based on a +0.25 diopter spherical reduction in each eye from a cycloplegic refraction conducted by the referring provider. The extraocular muscles showed full range of motion, but there were saccadic intrusions with small amplitude horizontal nystagmus, which dampened in right gaze and with convergence. There was not a notable latent component to the nystagmus. Amplitude of accommodation was significantly lower than expected for his age; however, accommodative response accuracy was normal. Cover testing through his spectacle prescription measured 6 prism diopters esophoria at distance and 14 prism diopters of left esotropia (90%) at near. The near esodeviation decreased to 10 prism diopters through a +2.00 diopter add, indicating a gradient accommodative convergence-to-accommodation ratio calculation of 2 prism diopters of convergence per diopter of accommodation. Further specific accommodative and binocular findings are listed in Table 2. A foveal reflex was not observed during the dilated ocular health evaluation. A 5-line raster optical coherence tomography was performed, which confirmed grade 1 foveal hypoplasia (see Figure 2).

In addition to the mild foveal hypoplasia, the diagnosis of anisometropic amblyopia was kept because of the relative reduction in visual acuity of the left eye compared with the right eye. Patching was not a preferred option in this case because of the nystagmus, bilateral reduction in acuity, and weak fusion responses. A bifocal was considered but not prescribed because of the newly obtained glasses, minimal reduction in near esodeviation with added lenses, and robust stereopsis. Vision therapy was conducted to improve visual acuity, enhance binocularity, and increase fusional abilities to enhance control of the intermittent esotropia at near. The efficacy of 21 sessions of in-office vision therapy can be appreciated by the significant improvements in acuity, accommodative, and binocular metrics listed in Table 2, along with specific vision therapy activities. There was also a qualitative reduction noted in the nystagmus amplitude and velocity compared with the initial visit and previous examinations as reported by the referring provider.
Case 3
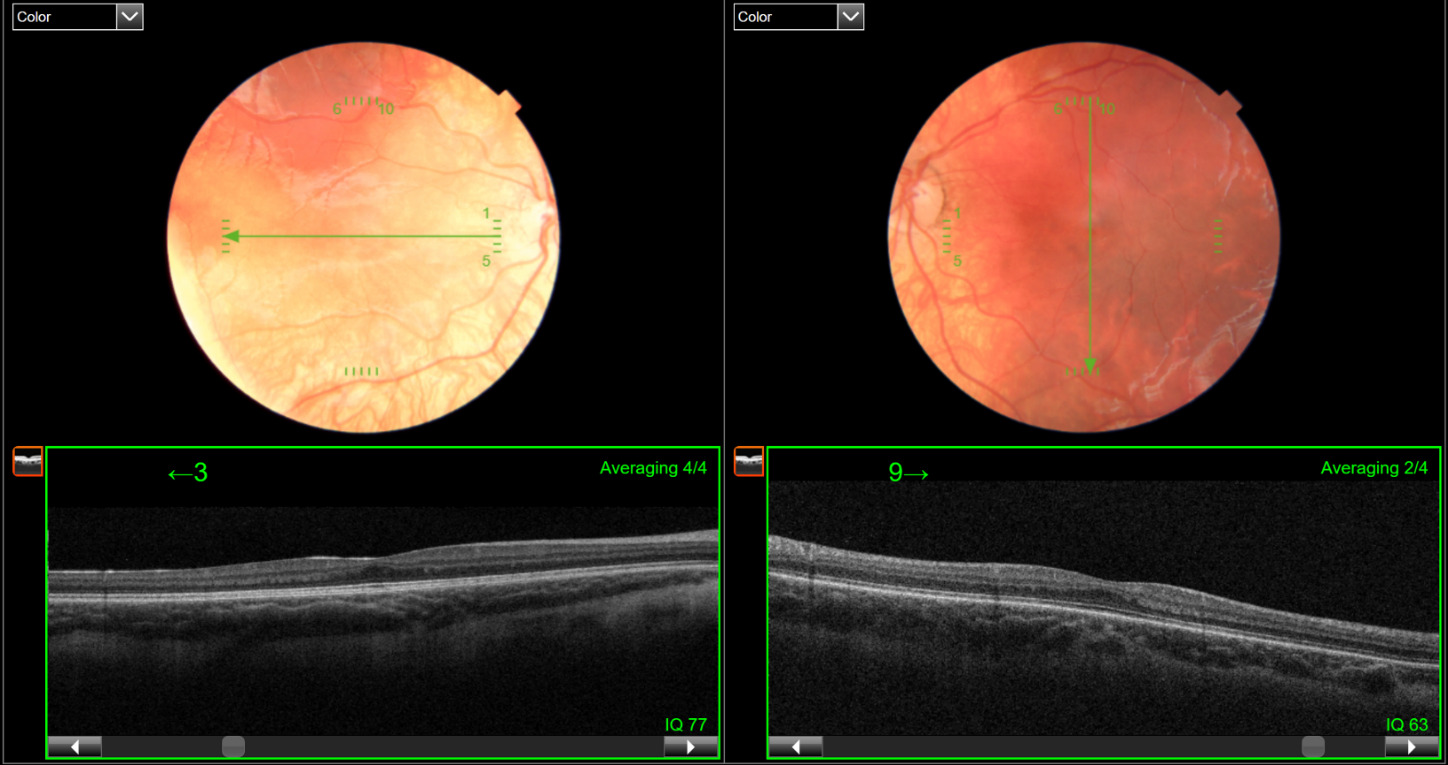
A 7-year-old boy presented for his annual examination to monitor his refractive amblyopia, secondary to hyperopic anisometropia and bilateral high astigmatism. Medical history was positive for Waardenburg syndrome type II, specifically a deletion of exons 5 through 9 of the MITF gene, a gene which can be associated with albinism.10,11 Waardenburg syndrome is associated with deafness and iris heterochromia, both of which were present in this patient. The patient had bilateral cochlear implants to address the hearing loss. Waardenburg syndrome is also frequently associated with a white forelock and large pupillary distance, which were not present in this patient but were present in his mother who also has been diagnosed with the condition. His parents expressed a desire to optimize his vision, especially given the language and speech delays secondary to his deafness. Measures of visual acuity from previous examinations had been inconsistent because of age, speech delays, and cooperation during the examinations. He had been in glasses with full hyperopic correction since age 3 years and had previously attempted patching, with a few sessions of vision therapy to improve visual acuity and stereopsis. At the current examination, best-corrected visual acuity measured using HOTV single letter with crowding bars was 20/40 in each eye. His habitual prescription was +3.75 -2.50 x 180 in the right eye and +5.25 – 2.50 x 001 in the left eye, with a +2.50 add for a previously diagnosed high esophoria at near. This prescription was based on cycloplegic retinoscopy, with the full hyperopic power incorporated to reduce the patient’s esophoric alignment. At this visit, cover test findings measured orthophoria at distance and 6 prism diopters of esophoria at near through the bifocal, without measurable random dot stereopsis. The patient was able to pinch the Stereofly wings above the page and exhibited fusion at all distances in dark and bright illumination with the Worth Dot test. The dilated fundus examination revealed bilateral hypopigmented fundi, which was more evident in the right eye. Given the poor improvement in acuities with prior amblyopia treatment and the fundus appearance, a 5-line raster optical coherence tomography was performed, which revealed grade 1 foveal hypoplasia in both eyes (see Figure 3). A pattern reversal visual evoked potential was also conducted to derive an objective estimate of the potential visual acuity of the patient, which enabled an assessment of the veracity of the subjective acuity measures. Potential visual acuity estimates were based on a regression model developed at the Michigan College of Optometry using the LKC 5-step pattern reversal visual evoked potential protocol.12 Results from the pattern visual evoked potential estimated a best-corrected visual potential of at least 20/30 binocularly. A full-field flash electroretinogram was also conducted, which ruled out cone- and rod-mediated retinal dysfunction. No further visual treatment was recommended at this time based on the cumulative results of clinical testing.

DISCUSSION
Amblyopia is commonly encountered in pediatric optometric practice, with rates estimated around 2% in the general population.13,14 The standard sequence of amblyopia treatment includes best optical correction, patching, and then more aggressive patching or binocular therapy if necessary.15 However, this sequence is complicated when there is a concurrent structural anomaly as a contributing cause of the reduced vision, such as foveal hypoplasia. Patching may be contraindicated in foveal hypoplasia with nystagmus, particularly with latent components, which may worsen visual acuity when a patch is used. A Bangerter foil as the occlusion method could have been attempted in cases 1 and 2, but the coexistence of strabismus for each case made vision therapy with targeted vergence and antisuppression training a better option for both, allowing a focus on simultaneous perception, improved peripheral or central fusion, and expanded vergence ranges. Home dichoptic technology is another excellent option for clinicians to consider for patients with foveal hypoplasia when monocular patching is not an option because of nystagmus, as home devices are approved for young children, maximize binocularity, are easy to administer at home, and are engaging for patients.16,17 Case 1 and 2 fell outside the strabismus parameters under current US Food and Drug Administration approval for devices that might otherwise be prescribed to the patient for home use, and the devices were not available at the time of these patient visits. With either home dichoptic therapy or in-office vision therapy, the binocular nature of the treatment and emphasis on improving binocularity through peripheral fusion rather than visual acuity alone may minimize the influence of any latent nystagmus associated with foveal hypoplasia, and improves stereopsis.16,17
Although not genetically confirmed, case 1 has a highly likely diagnosis of ocular albinism, with the classic ocular features of nystagmus, foveal hypoplasia, and high refractive error and the physical features of fair skin, hair, and ocular structures.6 Clinical pearls from this case are 2-fold. First, visual acuity can be improved in cases of foveal hypoplasia with coexisting amblyopia, especially with improvement of nystagmus. Second, fusion can be improved in cases of intermittent exotropia coexisting with foveal hypoplasia, and treatment such as vision therapy should be attempted if the patient is willing and motivated. This case also demonstrates the use of foveal hypoplasia staging as a guide and not a hardline endpoint of visual acuity potential. For case 1, the authors acknowledge that the improvements in visual acuity are likely attributed to the combined effects of vision therapy, the optical improvement of retinal image quality with the rigid gas-permeable contact lenses, and their possible effect of nystagmus dampening due to tactile feedback. However, there were also significant improvements in both motor and sensory fusion, underscoring the positive impact of vision therapy in this case.
Case 2 demonstrates that the visual outcome of foveal hypoplasia is dependent on the grade of hypoplasia present. In cases of low-grade foveal hypoplasia, with other amblyogenic factors present, improvements in visual acuity can be achieved with appropriate vision therapy approaches. As with the first case, vergence disorders can be treated concurrently in cases in which fovea hypoplasia is present. This case also highlights the importance of critically evaluating the amblyogenic factors and whether the reduced acuity aligns with the independent contributions of amblyogenic factors and foveal hypoplasia. When the acuity does not match the expected values based on the degree of foveal hypoplasia, further treatment should be attempted. In case 2, the anisometropic hyperopia was the minimum amount considered amblyogenic, and the intermittent and unilateral nature of the strabismus did not explain the reduced vision in both eyes. The optical coherence tomography was especially beneficial in this case to provide more clinical insight, but foveal hypoplasia staging predicted much better acuities than the presenting acuities. Therefore, it was prudent to initiate amblyopia treatment, which did in fact improve visual acuity posttreatment. The normal foveal development process of cone elongation and packing can occur up to age 13 years,18 which may explain the significant visual improvement in case 2 for both the sound eye and the amblyopic eye. It is well established that young children are less adept at performing visual acuity tasks, and preschool children tend to demonstrate lower acuity measures compared with older cohorts.19,20 Given this, it would be expected that the younger the patient and the less severe the foveal hypoplasia, the better improvements and final visual acuity would be expected, particularly over time. The Amblyopia Treatment Studies have demonstrated that although amblyopia treatment is possible in older children, treatment may take longer as compared with younger children.15 This may explain the significant improvement for case 2 given his younger age at treatment initiation.
Case 3 also highlights the importance of optical coherence tomography when amblyopia is not improving as expected with treatment and electrodiagnostic testing as follow-up when foveal hypoplasia is present. Given the degree of foveal hypoplasia and the corroboration with the visual evoked potential results, this was a reasonable endpoint for the patient at this age. Mild grades of foveal hypoplasia can be difficult to appreciate through standard examination protocol, because of poor patient fixation or highly reflective internal limiting membrane in children, complicating the view of the foveal light reflex. When performing optical coherence tomography scans, especially in patients with poor fixation or young age, a macular cube in addition to a line raster will enable a denser tomographic sampling of the macula region. Even though the 5-line raster scan is limited in its scan density, which increases the risk of missing the fovea, the faster rate of its scan acquisition may enable greater success in achieving useful foveal scans, specifically in patients with poor fixation or nystagmus. This was the reason the 5-line raster was performed for the patients in this case series, rather than the macular cube. Clinicians could consider either increasing the raster density of the 5-line scan or repeating scans at future visits to increase the probability of capturing the foveal region. Macular cubes may also help determine if acuity is reduced because of eccentric fixation, but that measurement was beyond the scope of this case series.21,22
Although various grades of foveal hypoplasia correspond to specific expected visual acuities, an absence of a foveal pit does not necessarily result in reduced vision.23,24 Visual acuity as an isolated marker of improvement is further complicated by the fact that younger children have lower expected visual acuity even in cases of normal vision and ocular development. The authors were confident in the reliability of the visual acuities in cases 1 and 2 because of patient ages, but case 3 may have taken longer to rule out foveal hypoplasia because of the slightly reduced visual acuity being attributed to age-expected norms instead of a pathological cause. Electrodiagnostic results are useful in predicting visual acuity potential and identifying cone-mediated inherited retinal diseases. Genetic testing is also useful in determining if there are systemic causes of the hypoplasia, such as ocular albinism or other pigmentary disorders.
CONCLUSION
Amblyopia can occur concurrently with ocular disease and structural abnormalities such as foveal hypoplasia. Imaging the fovea and grading the foveal hypoplasia in cases with amblyopia is a prudent approach, especially when developing a more informed prognosis for acuity improvement in such cases. Adjunctive testing with visual electrodiagnostics may provide additional insight into objective estimates of the visual potential and the integrity of retinal function. Patching may be contraindicated in amblyopia with nystagmus, especially if there is a latent component, so vision therapy aimed at acuity improvement and fusion enhancement should be considered in cases with foveal hypoplasia. The grade of foveal hypoplasia and motivation of the patient may influence the relative improvements expected with such intervention.
DISCLOSURES
No identifiable health information was included in this case series.
The authors declare no conflicts of interest.
The authors declare no funding sources.
ACKNOWLEDGEMENTS
The authors would like to acknowledge the following individuals for their roles in the clinical care in these cases: Maddie Seidel, OD, FAAO, and Alli Richardson, OD, FAAO. Dr McDowell would also like to thank Julie DeKinder, OD, FAAO for her thoughtful review and edits.