

INTRODUCTION
Central retinal vein occlusions are commonly seen in older adult patients, affecting both sexes equally.1,2 Risk factors include smoking, hypertension, diabetes mellitus, sleep apnea, and glaucoma.3–5 In younger patients, retinal vein occlusions may be associated with traditional vascular risk factors or nontraditional etiologies, such as thrombophilic disorders, inflammatory conditions, and possible drugs such as oral contraceptives. Both the anatomy of the lamina cribrosa and hemodynamic factors play a role in the pathogenesis of the condition.6 Individuals with central retinal vein occlusions may present with sudden, painless vision loss with clinical findings of venous dilation and tortuosity, retinal hemorrhaging in 4 quadrants, cotton wool spots, retinal edema, and/or optic disc edema.1 Management includes close monitoring for the development of potential complications such as neovascularization.7–9 Neovascularization may occur in the iris, angle, retina, and/or optic disc.9
The cilioretinal artery was first described by Mueller in 1856 as a congenital vascular variant that typically supplies the inner sensory retina, temporal to the optic disc.10–12 It arises from the ciliary vessels and is most commonly found on the temporal side of the disc.13 Cilioretinal artery occlusions are thought to occur secondary to a partial obstruction of the posterior ciliary arteries,6,14,15 though the exact pathogenesis remains unclear. Cilioretinal artery occlusion types include nonarteritic isolated cilioretinal artery occlusion, arteritic cilioretinal artery occlusion, and cilioretinal artery occlusion associated with a vein occlusion.6,16,17 Patients with cilioretinal artery occlusion may present with decreased vision, complaints of a scotoma in their vision, and/or clinical findings of retinal whitening due to retinal ischemia.6,16,18,19
Combined central retinal vein occlusions and cilioretinal artery occlusions represent uncommon vascular pathologies associated with the retina that can lead to acute and sometimes permanent vision loss. The first case was presented by Oosterhuis in 1968.20 Although pathophysiology is still controversial, Hayreh concluded that it is likely due to the impeded hemodynamic flow in the cilioretinal artery due to the central retinal vein occlusion.6
This case report highlights the clinical characteristics and pathogenesis of a combined central retinal vein occlusion and cilioretinal artery occlusion in a middle-aged patient with a medical history of pulmonary embolism and concurrent oral anticoagulant use. The patient was switched from warfarin (Coumadin) to apixaban (Eliquis) for convenience; however, improper anticoagulation management/effect likely contributed to the development of the occlusive event. The report also reviews current diagnostic technologies and treatment options while reviewing the implications of anticoagulation therapy in preventing similar retinal vascular events. No identifiable health information was included in this case report.
CASE REPORT
Initial Visit
A 42-year-old African American male patient presented to the urgent care eye clinic with complaints of sudden-onset blurry vision in the left eye with an accompanying “dark spot” in his vision. Symptoms started 6 hours earlier while at work. His last eye examination was 2 years ago and was unremarkable. His medical history was pertinent for hypertension and a pulmonary embolism that occurred in 2012. Current medication included only apixaban and a prior history of warfarin use. The patient was switched to apixaban 7 months prior because of the convenience of treatment and less frequent monitoring. The patient was not receiving hypertensive medications. He reported adherence to his medication and follow-up schedules.
The patient was alert and oriented to time and place. Corrected Snellen visual acuity was 20/20 in the right eye and 20/125 with no pinhole improvement in the left eye. Pupils were equal, round, and reactive to light with no relative afferent pupillary defect in either eye. Extraocular motilities were full in all gazes and confrontation visual fields were full to finger count in both eyes. Slit-lamp examination of the anterior segment was unremarkable in both eyes. Intraocular pressure measured 13 mm Hg in the right eye and 13 mm Hg in the left eye. The patient’s blood pressure was 134/87 mm Hg in-office. The dilated fundus examination was normal in the right eye (Figure 1). Fundus examination of the left eye demonstrated a swollen optic nerve, scattered cotton wool spots, intraretinal hemorrhages throughout the posterior segment, dilated and tortuous veins, and retinal whitening and inner retinal edema in the area of the cilioretinal artery (Figure 2). Neovascularization of the retina and optic nerve was not observed. Fundus photography and Zeiss CIRRUS spectral domain optical coherence tomography were completed. Optical coherence tomography showed hyperreflectivity and thickening of inner retinal layers and loss of inner retinal layer differentiation (Figure 3). The patient was diagnosed with a concurrent central retinal vein occlusion and a cilioretinal artery occlusion in the left eye.



Because of the presence of the cilioretinal artery occlusion and the inherent risk of stroke, the patient was immediately referred to the emergency department for a stroke evaluation. On admission, the patient’s prothrombin time and international normalized ratio were not obtained as patient was not treated with warfarin. Given current treatment with apixaban, a dilute Russell viper venom test and partial thromboplastin time were obtained, and both indicated delayed clotting time. A complete transthoracic echocardiogram with contrast revealed a left ventricular thrombus. The patient’s carotid duplex showed no evidence of hemodynamically significant stenosis. Magnetic resonance imaging of the brain was not recommended at that time. The patient was referred to hematology to reevaluate his current therapy. A subsequent examination with a retina specialist confirmed the retinal diagnosis and the patient received an intravitreal bevacizumab (Avastin) injection in the left eye.
Follow-Up Visit
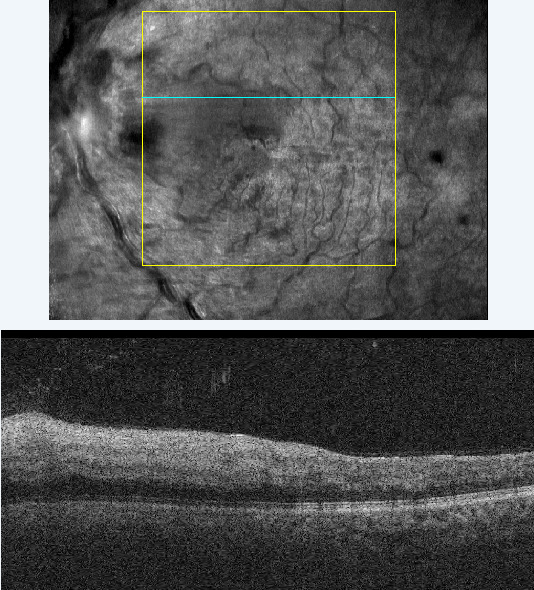
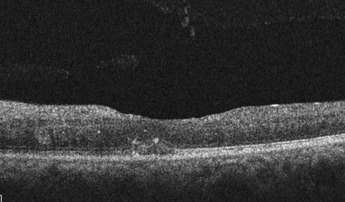
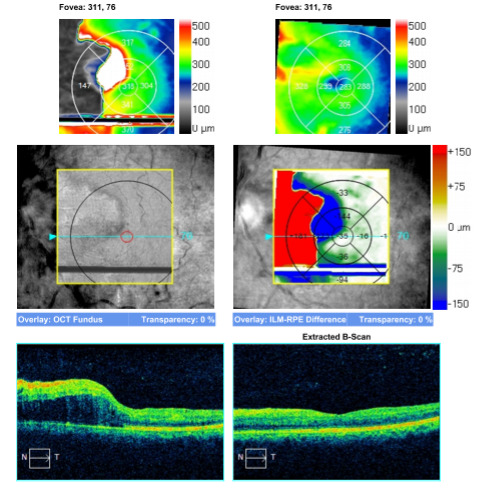
The patient returned 1 month later for a follow-up visit. He reported mild improvement in vision and good compliance with his primary care and hematology visits. His best-corrected vision was 20/50 in the left eye with no improvement on pinhole. Acuity in the right eye was stable at 20/20. Slit-lamp examination was unremarkable in both eyes. Optic nerve head swelling and intraretinal hemorrhages in the posterior segment improved from the initial visit, veins were dilated and tortuous, and the retinal whitening was no longer present. Optical coherence tomography was repeated, which revealed improved retinal edema (Figure 4) with underlying retinal pigment epithelium disruption. Macular change analysis showed improvement of edema at follow-up compared with the initial visit (Figure 5).


The patient was seen again over the course of a few months, with his final best-corrected acuity in the left eye being 20/40; the right eye remained stable to the initial examination. The retinal swelling resolved with residual retinal atrophy and thinning. No further bevacizumab injections were indicated. The patient was closely monitored for ocular complications associated with the central retinal vein occlusion and cilioretinal artery occlusion and did not develop neovascularization of the iris, angle, retina, or optic disc. As the patient failed treatment with apixaban, as evidenced by the development of the retinal thromboembolic event, he was switched back to warfarin with close monitoring of his prothrombin time, partial thromboplastin time, and international normalized ratio. Lifestyle modifications were discussed with the patient, and regular follow-ups with hematology, ophthalmology, and cardiology were recommended.
DISCUSSION
Although the pathophysiology of a combined central retinal vein occlusion and cilioretinal artery occlusion has been hypothesized, no definitive etiology has been confirmed. The combined ischemic event may be related to the partial obstruction of the posterior ciliary arteries.15 Schatz reviewed various causes, including how disc edema secondary to the vein occlusion may contribute to the artery occlusion.14 Hayreh proposed that the vein occlusion may cause a transient drop in perfusion pressure of the cilioretinal artery, leading to a secondary artery occlusion.6 He further stated this is likely a hemodynamic mechanism rather than an embolic or thrombotic etiology, explaining that perfusion pressure is arterial pressure minus venous pressure.6 Any reduction in arterial pressure or increase in venous pressure can result in reduced perfusion, leading to the ischemic event. Although the pathophysiology of a combined vein and artery occlusion has not been agreed on, a timely referral and appropriate management are key in these cases.
Acute artery occlusions require prompt referrals to the emergency department or stroke center to determine etiologies and to try to prevent cerebrovascular accidents. In this patient’s case, he was referred to the emergency department, where a battery of tests was completed. As the patient was not receiving warfarin, traditional tests such as prothrombin time and international normalized ratio were not completed. Although apixaban may alter results, these tests do not accurately measure its anticoagulant effect. Instead, a partial thromboplastin time and dilute Russell viper venom test were completed as these provide more meaningful clinical information in patients receiving apixaban. The latter is a screening test that is now crucial in detecting antiphospholipid antibodies, which are the most common cause of acquired thrombophilia.21 As the patient was receiving apixaban, these tests were deemed necessary. After switching the patient to warfarin, prothrombin time, partial thromboplastin time, and international normalized ratio were completed more frequently and were improved at the 6-month follow-up with hematology.
Apixaban is a novel oral anticoagulant that requires less frequent monitoring and provides the convenience of oral administration. However, in this case, the patient was unable to continue this medication and required switching back to warfarin. The patient’s care was reestablished with hematology, and the vision improved from the initial examination. Apixaban has a higher safety profile compared with warfarin, given a decreased risk of bleeding, stroke, systemic embolism, and fewer medication and food interactions.22–26 Unfortunately, the patient’s treatment with apixaban failed, requiring him to switch back to warfarin because of the occlusive event.
Management of central retinal vein occlusions and cilioretinal artery occlusions is directed toward complications once underlying systemic conditions have been thoroughly investigated. Artery occlusions are associated with increased morbidity, given the inherent risk of stroke.27,28 These must be managed as medical emergencies, and the systemic cause of the embolism must be identified. With vascular occlusive events, age may affect the differential diagnoses. In younger patients, hypercoagulable states, autoimmune or inflammatory vasculopathies, and medication-related causes, in addition to our traditional risk factors of hypertension, diabetes mellitus, hyperlipidemia, and glaucoma, must be ruled out. A thorough medical history and systemic workup to determine if hypercoagulopathies or inflammatory vasculopathies exist will help determine possible traditional vs nontraditional etiologies. Visual prognosis is related to the severity and duration of ischemia and the area of the fovea affected.6 Hayreh concluded that, in cases of cilioretinal artery occlusions, vision loss is attributed to swelling of the foveal retina secondary to the occlusive event.6 Although studies have investigated the efficacy of lowering intraocular pressure, ocular massage, and thrombolysis in cases of retinal artery occlusions, there is no proven therapy for visual recovery.29 Because of ocular ischemia, patients must be monitored for ocular complications related to neovascularization of the disc and iris.30
Ocular complications of central retinal vein occlusions are more commonly seen in ischemic events, but nonischemic or indeterminate occlusions may convert to ischemic occlusions.6 Ocular complications of central retinal vein occlusions include neovascularization and macular edema.7–9 Neovascularization may occur in the retina, optic disc, iris, or anterior chamber angle.9 Anterior segment neovascularization is the most serious complication of a central retinal vein occlusion and is normally proportionate to the level of ischemia present. Close observation is essential to rule out anterior segment neovascularization and prevent neovascular glaucoma. The prognosis of combined central retinal vein occlusions and cilioretinal artery occlusions is favorable, especially in younger patients.31 However, prognosis is impacted by the level of ischemia and whether the retinal infarct involves the foveal zone.6
Macular edema may occur in patients with central retinal vein occlusions and can be visually debilitating. If macular edema is noted, patients should be referred to a retinal specialist to determine the best treatment option. Various studies have evaluated the efficacy of intravitreal steroid injections, anti–vascular endothelial growth factor therapy, and grid panretinal photocoagulation in the treatment of central retinal vein occlusions. The Standard Care vs Corticosteroid for Retinal Vein Occlusion study found steroids to be effective in visual improvement, but complications outweighed benefits.32 The Ranibizumab for Macular Edema following Central Retinal Vein Occlusion study found anti–vascular endothelial growth factor medication to be effective in reducing macular edema and improving vision.33 COPERNICUS and GALILEO evaluated the efficacy and safety of aflibercept (Eylea) and supported the use of anti–vascular endothelial growth factor in the treatment of macular edema secondary to vein occlusions. BALATON and COMBINO evaluated the efficacy of faricimab (Vabysmo) vs aflibercept, concluding faricimab was well tolerated and noninferior to aflibercept. The Central Vein Occlusion Study found that although grid laser reduced macular edema, vision did not improve, and panretinal photocoagulation did not prevent neovascularization in these cases.34 Currently, anti–vascular endothelial growth factor remains the front-line treatment for macular edema secondary to central retinal vein occlusions. First-line agents for macular edema secondary to vein occlusions include aflibercept, bevacizumab, and ranibizumab (Lucentis).
CONCLUSION
This case demonstrates a combined central retinal vein occlusion and cilioretinal artery occlusion in a middle-aged patient with a history of pulmonary embolism following a change in systemic medication. In all patients presenting with a vein occlusion, macular edema and neovascularization must be ruled out. Acute artery occlusions represent a medical emergency, and the etiology must be determined. With the patient’s history of pulmonary embolism, the etiology was clear, but further investigation was necessary to determine why the patient’s anticoagulation was not controlled with his current treatment. After determining the patient failed current treatment with apixaban, he was switched back to warfarin, and his anticoagulative effects were controlled.
TAKE HOME POINTS
-
Combined central retinal vein occlusions and cilioretinal artery occlusions are rare and likely a complication of a patient’s underlying systemic conditions.
-
Retinal artery occlusions are medical emergencies, and prompt referral is crucial.
-
Close monitoring is key to detect ocular complications such as neovascularization.
Disclosures
No identifiable health information was included in this case report
The author declares no conflicts of interest
The author declares no funding sources