INTRODUCTION
Optic neuropathies encompass damage to the optic nerve caused by various factors and can be categorized into several main groups based on etiology: ischemic, inflammatory/demyelinating, compressive, hereditary, toxic/nutritional, traumatic, infectious, and autoimmune.1,2 "Iatrogenic" refers to optic nerve damage caused by medical treatment or medications.3 Drug-induced optic neuropathies are often categorized based on their underlying pathophysiology. Medications like ethambutol and amiodarone can cause toxic optic neuropathies through direct mitochondrial damage to the optic nerve, not inflammatory mechanisms.1,4 As oncology treatments expand, new agents cause ocular side effects. Optic neuropathies from immune checkpoint inhibitors are autoimmune, involving immune-mediated optic nerve inflammation similar to classic autoimmune optic neuritis, classified as immune-related adverse events.2
The landscape of cancer treatment has transformed dramatically with immune checkpoint inhibitors. Anticytotoxic T-lymphocyte-associated protein 4 was approved in 2011 as a type of immune checkpoint inhibitor to treat advanced melanoma. Since then, immune checkpoint inhibitor eligibility has surged from 40% of US cancer patients in 2019 to more than 56% of those with advanced or metastatic disease by 2023.5,6 The American Society of Clinical Oncology now recognizes immune checkpoint inhibitors as standard care across multiple solid-organ and hematologic malignancies, with new agents and combination therapies continuously expanding their clinical applications.5 Among these immune checkpoint inhibitors, nivolumab (OPDIVO 10 mg/mL, Bristol-Myers Squibb Company) is a programmed death receptor-1 blocking antibody increasingly used to treat advanced melanoma, non–small cell lung cancer, and other carcinomas.7
This case highlights presumed autoimmune/inflammatory optic neuropathy as a rare side effect of nivolumab, an immune checkpoint inhibitor. It also underscores the importance of prompt workup and referral when presented with bilateral disc edema in an acute presentation of optic neuropathy to rule out life-threatening conditions.
CASE REPORT
A 58-year-old woman with advanced metastatic melanoma (stage IV) was treated with nivolumab 10 mg/mL injectable solution for 6 months with minimal side effects. The melanoma was responding well to the nivolumab treatment. After 6 months of therapy, she noticed visual disturbances and clouding in the inferior portion of her vision in her left eye. She presented to the optometry clinic for evaluation 2 days after symptom onset, describing progressively worsening visual distortion and clouding. The patient denied symptoms of headache or eye pain. Her medical history included breast cancer and hypothyroidism but no underlying vascular conditions. Her breast cancer had been successfully managed with surgical excision 6 years prior.
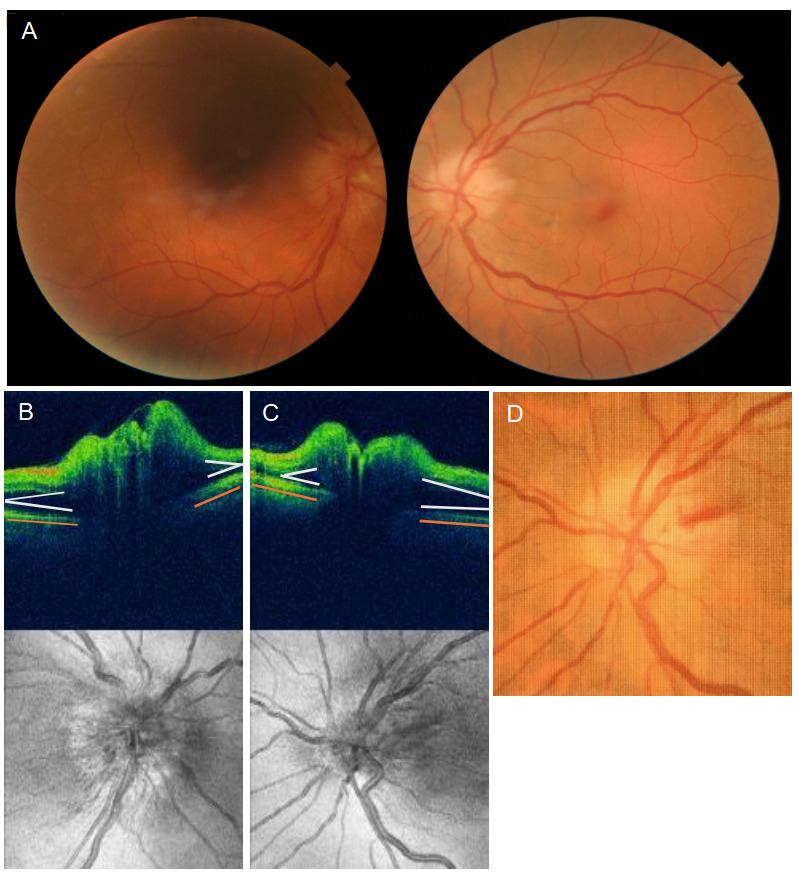
Her medications included levothyroxine (250 mg) and nivolumab injection (250 mg every 2 weeks). The best-corrected distance visual acuity was 20/25 in the right eye and 20/100 in the left eye. Extraocular motilities were normal. Confrontation visual fields testing revealed an inferior field defect in the left eye, with no abnormalities detected in the right eye. The pupillary response was normal pupillary response in the right eye and a 2+ relative afferent pupillary defect in the left eye (clinical plus scale). Posterior segment findings revealed significant optic disc edema with an optic nerve cup-to-disc ratio of 0.1 round in both eyes. The optic disc edema was graded as Frisen 1 in the right eye and Frisen 2 in the left eye. Fundus photography was acquired at the beginning of the examination documenting the bilateral optic disc edema. Within 20 minutes of obtaining the initial fundus photograph and acquiring optical coherence tomography imaging, a prominent optic disc hemorrhage developed on the temporal rim of the left optic disc. Optical coherence tomography (Cirrus HD-OCT 4000, Carl Zeiss Meditec Inc) showed elevated optic disc tissue with a “lazy V sign” contour formed by a subretinal hyporeflective space adjacent to the optic nerve head and additionally had a flat-V peripapillary retinal pigmented epithelium/Bruch’s membrane contour (Figure 1). The “lazy V sign” is an optical coherence tomography finding suggestive of disc edema, whereas the flat-V peripapillary retinal pigmented epithelium/Bruch’s membrane contour is a finding that suggests normal intracranial pressure.8–10

Fundus photography was used to document the development of the disc hemorrhage in the left eye (Figure 1). The rapid development of the optic disc hemorrhage indicated acute optic nerve changes, necessitating immediate neuroimaging to rule out life-threatening conditions. Visual field testing was not performed at this initial visit because the commercial optometry practice did not have an automated perimeter on site. The patient was promptly sent to the emergency department for same-day imaging and a full workup.
Once admitted to the emergency department, the patient underwent comprehensive evaluation to systematically address the differential diagnosis of bilateral optic disc edema, including papilledema, ischemic optic neuropathy, inflammatory conditions, infectious etiologies, and iatrogenic causes. This workup included magnetic resonance imaging with and without contrast of the brain and orbits, laboratory studies, and lumbar puncture. The results of the magnetic resonance imaging showed no tumors, malformations, obstructions, or magnetic resonance imaging features of increased intracranial pressure. Detailed review of the magnetic resonance imaging showed bilateral enhancement of the optic nerves, which could be suggestive of an inflammatory cause for the bilateral optic disc edema, such as optic neuritis or an autoimmune/inflammatory optic neuropathy. There were no white matter lesions visualized, which would be typical of demyelinating conditions like multiple sclerosis. There were no magnetic resonance imaging findings to suggest other differential diagnoses such as increased intracranial hypertension, cerebral venous sinus thrombosis, hydrocephalus, or meningitis. The emergency room physician did not order a magnetic resonance venography and did not provide a reason why one was not ordered. Her blood work was routine, including normal erythrocyte sedimentation rate, C-reactive protein, and platelet count. The differential diagnosis of giant cell arteritis was ruled out based on normal inflammatory markers; therefore, a temporal artery biopsy was not performed. The patient was kept overnight in the hospital for additional testing and observation. A lumbar puncture was performed in the morning, which resulted in no abnormalities in the cerebrospinal fluid and normal opening pressure of 12 cm H₂O. Typically, an opening pressure above 25 cm H₂O is considered elevated and supports the diagnosis of raised intracranial pressure.11 The emergency room physicians and neurologist met with the patient’s oncologist to discuss the possibility of nivolumab causing the bilateral disc edema since imaging and testing were unremarkable. The diagnosis of exclusion was presumed iatrogenic, inflammatory/autoimmune optic neuropathy as a rare side effect of nivolumab. After the immune-related adverse event was identified, the difficult decision was made to take the patient off nivolumab to prevent further optic nerve damage and vision loss. The patient received intravenous methylprednisolone 1 g daily for 3 days during hospitalization to treat the acute optic neuropathy, as early intervention was critical to minimize irreversible long-term ocular damage. Upon discharge on day 3, she was prescribed oral prednisone 50 mg daily for 1 week followed by a tapering schedule.
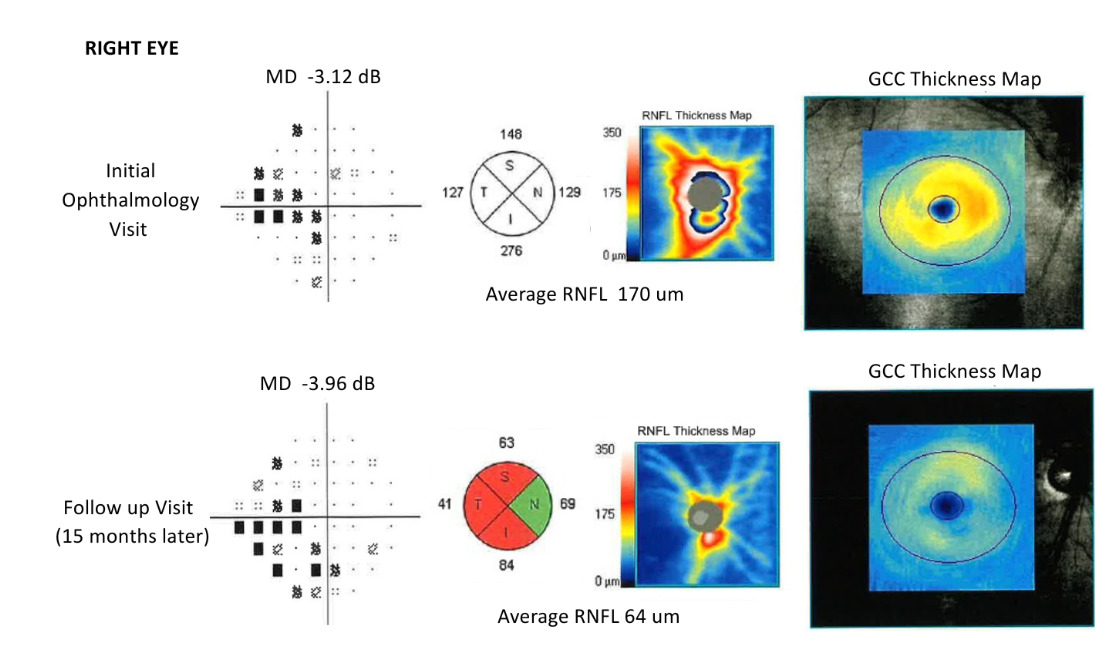
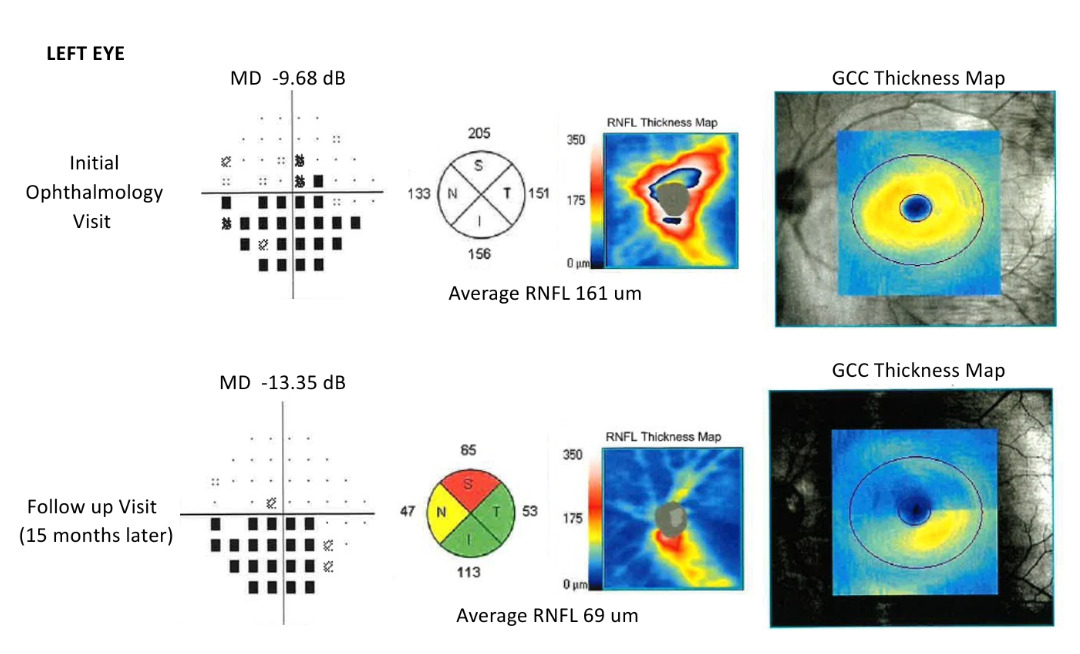
The patient had her first follow-up appointment with ophthalmology 9 days after leaving the hospital; she reported unchanged symptoms. She reported that the persistent blurry vision in the left eye had not worsened. She confirmed that her oncologist decided to discontinue nivolumab injection therapy because it was causing her bilateral optic disc edema. She reported that she was taking oral prednisone 50 mg daily but was starting the taper schedule dictated by her oncologist. Her best-corrected visual acuity had improved slightly, with 20/20-2 in the right eye and 20/80 in the left eye. The anterior segment was within normal limits, and the posterior segment showed residual elevation and blurred margins of the optic discs in both eyes. Optical coherence tomography (Cirrus HD-OCT 4000, Carl Zeiss Meditec Inc) showed elevation of the retinal nerve fiber layer and abnormal thickening of the neuroretinal rim in both eyes (Figures 2 and 3). Visual field testing (Humphrey Field Analyzer, Carl Zeiss Meditec, Inc) resulted in a nasal step in the right eye and a dense inferior arcuate scotoma in the left eye (Figures 2 and 3). Since the patient’s medication, nivolumab, was found to be the offending agent causing the optic disc edema, the plan was to continue monitoring the condition for improvement with serial perimetry.


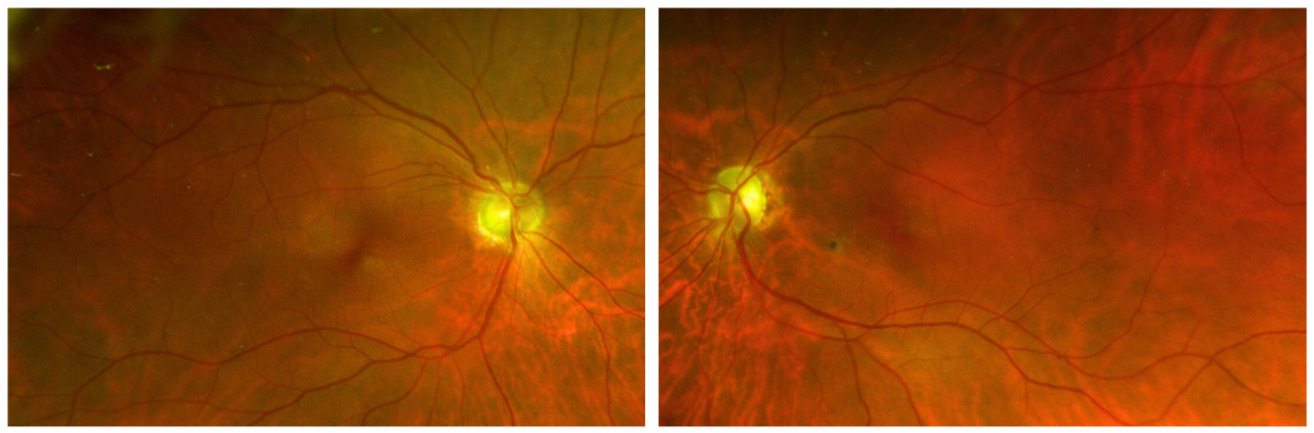
Over multiple visits, the patient’s visual acuity and optic disc edema showed gradual improvement. At the last follow-up visit, the optic nerves had stabilized approximately 15 months after the onset of ocular symptoms, resulting in atrophy and retinal nerve fiber layer thinning on the optical coherence tomography. Although the best-corrected visual acuities returned to normal, the patient had residual visual field defects in both eyes. The right eye showed a dense inferior nasal step, and the left eye showed a dense inferior arcuate scotoma. Figures 2 and 3 chronicle the pathophysiological progression from acute optic disc edema to subsequent optic atrophy with resultant permanent visual field defects over a 15-month observation period. Both eyes exhibit the characteristic pattern of initial neural tissue thickening followed by significant retinal nerve fiber layer thinning, accompanied by corresponding functional visual field defects that persisted after stabilization of the optic neuropathy. Figure 4 shows bilateral fundus photographs (Optos PLC) depicting the resolution of optic disc edema and subsequent development of optic atrophy at this follow-up evaluation. Both optic discs demonstrated temporal pallor, representing permanent structural sequelae of the preceding inflammatory process. The right eye showed moderate diffuse pallor in the superior, inferior, and temporal quadrants of the optic nerve, whereas the left eye demonstrated moderate to severe pallor in the superior and nasal quadrants of the optic nerve, correlating with the visual field defects. All other examination findings remained unchanged, including afferent and efferent pupillary responses and anterior and posterior segment findings, except for gradual resolution of bilateral disc edema. The retinal vasculature demonstrated normal caliber and distribution patterns against the background of the altered neuroretinal rim architecture. The resolution of the previously documented edema correlates with the optical coherence tomography findings that demonstrated significant reduction in retinal nerve fiber layer thickness from initial presentation to final assessment.

Despite long-term residual visual field defects, the patient was fortunate that her visual acuity returned to baseline levels. For long-term management of her advanced metastatic melanoma, the patient remained off nivolumab injection therapy and was switched to alternative medication to preserve her ocular health.
DISCUSSION
Iatrogenic optic neuropathy is a rare but serious adverse effect of certain medications, including anticancer medications. Nivolumab is an immune checkpoint inhibitor used primarily for treating advanced melanoma and other malignancies.2,7 Although it has been associated with various immune-related adverse effects, this case highlights a rare instance of presumed nivolumab-induced optic neuropathy.
The patient’s presentation of acute bilateral optic disc edema without other systemic symptoms posed a diagnostic challenge. A comprehensive evaluation was necessary to rule out more common causes of optic neuropathy, such as ischemic, infectious, inflammatory, or intracranial pathologies.3 The rapid development of an optic disc hemorrhage during the initial examination further emphasized the need for urgent investigation and prompt referral to get further neuroimaging and workup at the local hospital.
The differential diagnosis of bilateral optic disc edema encompasses several conditions that required systematic evaluation in this case including papilledema secondary to raised intracranial pressure, nonarteritic ischemic optic neuropathy, arteritic ischemic optic neuropathy, and optic neuritis.
Papilledema secondary to raised intracranial pressure was a primary consideration, as it represents the most common cause of bilateral disc swelling and can be life-threatening if caused by intracranial mass lesions or impaired cerebrospinal fluid outflow. This was effectively ruled out by magnetic resonance imaging findings that did not indicate increased intracranial pressure and lumbar puncture opening pressure of 12 cm H₂O, well below the threshold of 25 cm H₂O that would suggest intracranial hypertension.11 Optical coherence tomography imaging was suggestive of optic disc edema in the presence of normal intracranial pressure.
The optical coherence tomography from the initial visit (Figure 1B and 1C) provided 2 key diagnostic findings. First, it demonstrated the “lazy V sign”—a sideways V-shaped configuration of the retinal pigment epithelium/Bruch’s membrane layer with peripapillary tissue displacement forward, suggesting disc edema rather than pseudoedema conditions like optic disc drusen, where optic nerve elevation occurs without surrounding tissue alternation.8,9,12 This sideways V pattern should be distinguished from the second key diagnostic optical coherence tomography finding which is the peripapillary contour. The patient’s optical coherence tomography showed an upright V-shaped or flat contour that represents the normal peripapillary retinal pigmented epithelium/Bruch’s membrane configuration around the optic nerve. This flat-V configuration is suggestive of normal intracranial pressure, as elevated intracranial pressure typically produces anterior deformations with W-shape, S-shape, or dome configurations on optical coherence tomography.8–10
Ischemic optic neuropathy, particularly nonarteritic anterior ischemic optic neuropathy, was highly considered but deemed unlikely given the bilateral initial presentation and absence of typical vascular risk factors. The pathophysiology of nonarteritic anterior ischemic optic neuropathy is primarily vascular insufficiency at the optic nerve head, typically in patients with vascular risk factors and a “disc at risk” anatomy. In contrast, optic neuropathy associated with immune checkpoint inhibitors such as nivolumab is most often inflammatory or demyelinating in nature, resulting from immune-related adverse events rather than primary ischemia.13 Although some medications have been implicated in rare cases of nonarteritic anterior ischemic optic neuropathy, the literature does not support a direct mechanistic link between nivolumab and bilateral nonarteritic anterior ischemic optic neuropathy. Instead, reported cases of optic neuropathy with nivolumab are typically immune-mediated, sometimes presenting as optic neuritis or perineuritis, and are thus classified as iatrogenic (treatment-induced) but not as nonarteritic anterior ischemic optic neuropathy.12,14–16 The distinction is clinically important, as management and prognosis differ significantly between these entities.
Arteritic ischemic optic neuropathy or giant cell arteritis was systematically excluded based on normal inflammatory markers and clinical presentation (no jaw claudication, scalp tenderness, or weight loss), obviating the need for temporal artery biopsy.12
Infectious etiologies were excluded by normal cerebrospinal fluid findings and lack of systemic signs of infection.
The bilateral optic nerve enhancement on magnetic resonance imaging initially raised suspicion for inflammatory conditions, particularly optic neuritis associated with demyelinating diseases such as multiple sclerosis. However, the absence of multiple white matter brain lesions, normal cerebrospinal fluid analysis, and lack of systemic neurological symptoms effectively excluded classic optic neuritis.
Understanding the pathophysiology of nivolumab-induced optic neuropathy became crucial in establishing the correct diagnosis. This condition is immune-mediated, often presenting with features of optic neuritis or perineuritis, and is characterized by inflammation that frequently demonstrates enhancement of the optic nerve or sheath on magnetic resonance imaging with a favorable response to immunosuppressive therapy such as corticosteroids.16,17 This inflammatory profile is fundamentally distinct from nonarteritic anterior ischemic optic neuropathy, which represents a vascular, noninflammatory process resulting from hypoperfusion of the optic nerve head that is typically not responsive to steroids and lacks optic nerve enhancement on imaging. Importantly, nivolumab-induced optic neuropathy is best classified as an immune checkpoint inhibitor-induced optic neuropathy, specifically an inflammatory or autoimmune optic neuropathy, rather than a form of bilateral nonarteritic anterior ischemic optic neuropathy, optic neuritis, or bilateral papillitis. Although nivolumab-induced cases may mimic these traditional conditions, they are specifically triggered by immune checkpoint inhibition and can present with atypical features, including bilateral involvement and association with other immune-related adverse events.12,15–18
With these more common causes systematically ruled out and given the temporal relationship between nivolumab treatment and symptom onset, nivolumab-induced inflammatory/autoimmune optic neuropathy became the most likely diagnosis.
At the molecular level, nivolumab binds programmed death receptor-1 receptors on T cells, blocking interaction with PD-L1/PD-L2 ligands. This removes immune checkpoints that normally limit T-cell activation, enhancing antitumor immune responses.19 When patients develop optic disc edema after nivolumab treatment, it is considered an immune-related adverse event. The same mechanism that helps fight cancer—disruption of normal immune regulation—can trigger inflammation in noncancerous tissues. In the optic nerve, this can cause inflammation of the nerve itself (optic neuritis) or surrounding tissues (perineuritis), resulting in optic disc edema. This explains how nivolumab’s therapeutic effects against tumors can simultaneously cause unwanted inflammatory reactions in neural tissues.17,20,21 This mechanism aligns with the observed pattern in our patient, where nivolumab likely triggered an autoimmune response targeting optic nerve tissue.17,21,22
In addition to optic neuropathy and optic disc edema, other neuro-ophthalmic manifestations have been documented as ocular immune-related adverse events associated with immune checkpoint inhibitors, including cranial nerve palsies (most notably involving cranial nerve III, VI, VII, and VIII), neuromuscular junction dysfunction (particularly myasthenia gravis), and inflammatory orbital disease (such as orbital inflammation and orbital myositis). Less commonly reported ocular immune-related adverse events include neuroretinitis, immune retinopathy, and serous retinal detachment.22,23
Recent literature shows immune checkpoint inhibitor-related optic neuropathy occurs in less than 1% of patients in clinical trials, with serious neurologic immune-related adverse events in approximately 0.93% of nivolumab-treated patients. However, real-world ocular toxicities may be underreported due to lack of routine ophthalmologic screening.24–26
Current management guidelines from the European Society for Medical Oncology recommend discontinuing the immune checkpoint inhibitor and initiating high-dose corticosteroids as first-line treatment for severe immune-related adverse events.24,27 Following these guidelines, our patient received high-dose corticosteroids to treat the bilateral optic disc swelling, which proved effective, thereby supporting the diagnosis of inflammatory/autoimmune nivolumab-induced optic neuropathy. It is important to have early recognition and prompt intervention in managing neuro-ophthalmic manifestations of immune checkpoint inhibitors.28 In cases where corticosteroids are ineffective, additional immunosuppressive therapies may be considered.
Although specific demographic factors predisposing patients to nivolumab-induced optic neuropathy remain undefined, several risk factors warrant consideration. Patients receiving combination therapy of nivolumab and ipilimumab have a higher incidence of severe immune-related adverse events compared with those receiving nivolumab alone.24 Additionally, patients with metastatic melanoma who respond well to immunotherapy may be more likely to develop ocular complications.26
Regular ophthalmic screening is crucial for early detection of ocular adverse events. Recent publications highlight the importance of baseline and periodic ocular assessments in patients receiving immune checkpoint inhibitors to identify early signs of intraocular inflammation and other ocular toxicities.21 Although this patient’s visual acuity eventually improved, the persistence of visual field defects highlights the potential for lasting visual impairment. It has been noted that toxic optic neuropathies can improve after discontinuing the offending agent, but recovery may be incomplete depending on dosage and duration of exposure.3 Early recognition and intervention are crucial to minimizing permanent damage.
Given the increasing use of immune checkpoint inhibitors in oncology, awareness of their potential neuro-ophthalmic adverse effects is essential for early detection and intervention. Future studies and case reports will be necessary to understand better the incidence, risk factors, and management of nivolumab-induced optic neuropathy as more cases are reported.
CONCLUSION
Optic disc edema may indicate acute changes in the optic nerve and necessitate a thorough and prompt evaluation by clinicians to exclude life-threatening conditions. When faced with acute bilateral optic disc edema, it is crucial to conduct a comprehensive workup and diagnostic testing to identify alternative etiologies. The causes of optic disc elevation can range from increased intracranial pressure and ischemia to inflammation and various pseudoedematous conditions. With the increasing use of immune checkpoint inhibitors like nivolumab in oncology, awareness of their potential neuro-ophthalmic adverse effects is essential for early detection and intervention. Implementing standardized screening protocols, including baseline and periodic ophthalmic assessments, could help identify subtle changes before they progress to symptomatic disease. Timely and accurate diagnosis empowers physicians to modify treatment strategies, including the potential discontinuation of any offending medications, thereby mitigating the risk of permanent ocular damage. Notably, clinician awareness of optic neuropathy as a rare side effect of nivolumab is essential for its early recognition and effective management, ensuring optimal patient outcomes.
-No identifiable health information was included in this case report
-The author declares no funding sources.
-The author declares no conflict of interest.
TAKE HOME POINTS
-
Immune checkpoint inhibitors, including nivolumab, can cause iatrogenic optic neuropathy. With the increasing use of these medications in oncology, awareness of their potential neuro-ophthalmic adverse effects is essential for early identification and intervention.
-
Implementing standardized screening protocols, including baseline and periodic ophthalmic assessments for patients on immune checkpoint inhibitors, could help identify subtle changes before they progress to symptomatic disease.
-
Clinicians should have awareness for the potential change of signs or symptoms during their examination. In this case, rapidly progressing optic disc edema caused a new onset disc hemorrhage within 20 minutes.
-
When managing bilateral optic disc edema, comprehensive workup (which could include neuroimaging, lumbar puncture, and laboratory testing) is essential to rule out more common causes of optic neuropathy before attributing it to medication toxicity.
ACKNOWLEDGMENTS
The author would like to acknowledge Kristin Bretz, MD.