_revealing_cot.tiff)
__3-month_follow-.tiff)
__3-month_follow-u.tiff)
__3-month_fo.tiff)

INTRODUCTION
Purtscher retinopathy is an occlusive microvasculopathy associated with cranial trauma, chest compression, or long-bone fractures leading to retinal ischemia.1–3 In the absence of trauma, the term Purtscher-like retinopathy is used.1–3 Frequent causes of Purtscher-like retinopathy include acute pancreatitis, renal failure, and autoimmune disease like systemic lupus erythematosus.1,2 Because Purtscher and Purtscher-like retinopathies share clinical characteristics, the two entities are frequently discussed in tandem in the literature.1–3 Agrawal and McKibbin reported the incidence of Purtscher retinopathy (including Purtscher-like retinopathy) as 0.24 persons per million per year, but the incidence is likely higher given many patients are asymptomatic.3,4
Paracentral acute middle maculopathy was first introduced in 2013 and described as paracentral hyperreflective bands at the level of the middle retina on optical coherence tomography representing infarction of the inner nuclear layer.5 The current use of optical coherence tomography in routine clinical care has led to increased awareness and prompt diagnosis of paracentral acute middle maculopathy.6–8 Paracentral acute middle maculopathy develops from impaired perfusion of the deep retinal vascular complex.6,7,9 Like a cotton wool spot, paracentral acute middle maculopathy is a hallmark of an underlying condition.6,7 In fact, paracentral acute middle maculopathy may be the only ocular sign of carotid disease or giant cell arteritis.7,9–11 Thus, determining the etiology of paracentral acute middle maculopathy is essential in its management.7,9 In cases in which the etiology is unclear, the patient should be referred for urgent stroke evaluation.7,10,11
The aim of this report is 2-fold. First, a case of Purtscher retinopathy with concurrent paracentral middle maculopathy will be described. To our knowledge, this is the fifth report of Purtscher retinopathy with simultaneous paracentral acute middle maculopathy.12–15 Second, the causative factors, symptoms, clinical features, diagnostic evaluation, and evidence-based treatment for Purtscher retinopathy and paracentral acute middle maculopathy will be discussed. No identifiable health information was included in this case report.
CASE PRESENTATION
Initial Presentation
A 23-year-old White male presented for an urgent examination for blurry vision in both eyes and paracentral visual disturbances in both eyes following a motor vehicle accident in which he was riding a bicycle and was struck by the vehicle going 35 miles per hour. The accident occurred 1 month prior to his presentation to the eye clinic; because of his hospitalization, this was his first eye examination since the accident. He experienced loss of consciousness at the time of the accident and sustained significant injuries, including a laceration to the forehead, concussion, left orbital wall fracture, bilateral leg fractures, and complex laceration to the left hip/flank area with significant blood loss, for which he had been hospitalized. Per review of the medical record from the time of the accident, the complete blood count with differential revealed low erythrocyte count (2.83 M/µL, reference range: 4.30-6 M/µL), low hemoglobin (8.4 g/dL, reference range: 13.5-17 g/dL), and low hematocrit (25.1%, reference range: 40-53%). Although chest compression/contusion was not noted when reviewing the hospitalization records, it can be inferred based on the type of accident and other injuries sustained. Additional medical history was significant for left knee pain and hypercalcemia. He reported taking the following medications: multivitamins and zinc. He reported no known medical allergies. Family history was negative for ocular conditions. He was oriented to time, place, and person, with pleasant affect.
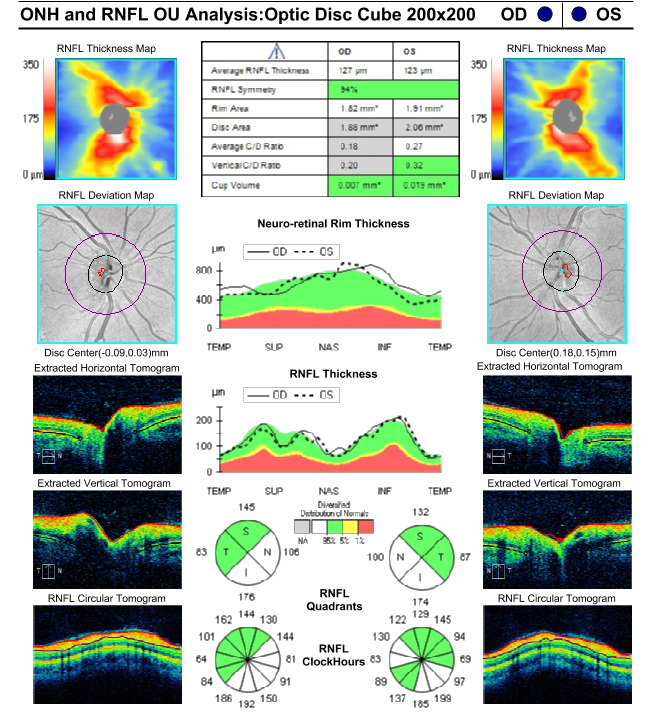
Best-corrected visual acuities were 20/20-1 right eye and 20/20-1 left eye. Pupils were equally round and reactive to light without an afferent pupillary defect. Extraocular movements were smooth and full in both eyes. Confrontation visual fields were full to finger counting in each eye. Amsler grid testing revealed a small area of metamorphopsia temporal to fixation in the right eye and small areas of metamorphopsia nasal and superotemporal to fixation in the left eye. Red cap testing was equal between the eyes. Slit lamp examination of the anterior segment was unremarkable in both eyes. Intraocular pressures by Goldmann applanation tonometry measured 14 mm Hg in each eye. Dilated fundus examination revealed a cup-to-disc ratio of 0.25 in each eye with well-perfused neural retinal rim tissue without edema or pallor. Examination of the posterior pole revealed mild retinal whitening superotemporal to the fovea in both eyes, a cotton wool spot in the inferior nasal arcade and a cotton wool spot in the inferior temporal arcade of the right eye, and 2 cotton wool spots in the superior temporal arcade of the left eye (Figure 1). The arterial-to-venous ratio was 2/3 in both eyes with no vascular tortuosity and no visible emboli. The peripheral retina was flat without holes, tears, or breaks in both eyes. Optical coherence tomography of the retinal nerve fiber layer revealed thick retinal nerve fiber relative to the normative database (not indicative of subclinical edema but rather due to his young age) inferiorly and nasally in both eyes with average retinal nerve fiber layer thickness of 127 microns in the right eye and 123 microns in the left eye (Figure 2). Optical coherence tomography showed central subfoveal thickness of 275 microns in the right eye (Figure 3A) and 271 microns in the left eye (Figure 4A). There were parafoveal hyperreflective bands in the inner nuclear layer worse in the right eye (Figure 3B) compared with the left eye (Figure 4B). En face optical coherence tomography at the level of the mid-retina showed patchy hyperreflectivity worse in the right eye (Figure 3C) compared with the left eye (Figure 4C), which corresponds to the inner nuclear layer hyperreflectivity on cross-section. Interestingly, in this case, there is also hyperreflectivity of the internal limiting membrane superotemporal to the fovea in both eyes (Figures 3D and 4D, right and left eye, respectively) that corresponds to the areas of retinal whitening seen on fundoscopy. The superficial capillary plexus on optical coherence tomography angiography showed an abnormal foveal avascular zone with small patches of capillary dropout worse in the left eye (Figure 5C) compared with the right eye (Figure 5A); the deep capillary plexus showed multifocal ovoid areas of signal attenuation due to capillary dropout in both eyes (Figures 5B and 5D, right and left eye, respectively).
_revealing_cot.tiff)
_at_initial_presentati.png)
__3-month_follow-.tiff)
__3-month_follow-u.tiff)
__3-month_fo.tiff)
Based on the patient’s medical history and clinical findings, Purtscher retinopathy with concurrent paracentral acute middle maculopathy in both eyes was the leading diagnosis causing the symptom of paracentral visual distortions. Other differential diagnoses considered were hypertensive retinopathy, diabetic retinopathy, human immunodeficiency virus retinopathy, and retinal vascular occlusion. The patient’s most recent blood pressure was 127/77 mm Hg 1 week prior to his presentation to the eye clinic, his most recent glycosylated hemoglobin A1c was 4.9% 7 months prior to his presentation to the eye clinic, and he had a negative human immunodeficiency virus test 3 years prior without high-risk behaviors such as intravenous drug use or unprotected sex. Retinal vascular occlusion was low on the differential list because of the bilateral presentation and lack of retinal hemorrhages. He was informed of the natural history of Purtscher retinopathy and paracentral acute middle maculopathy and was asked to return to the eye clinic in 4 weeks. In this case, the cause of Purtscher retinopathy is multifactorial, including head trauma, bilateral leg fractures, and probable chest trauma following a motor vehicle accident in which a car travelling 35 miles per hour struck the patient on a bike.
Subsequent Follow-Up Visits
He was monitored at 4-week intervals but was lost to follow-up after the 3-month visit. Visual acuity improved to 20/20 in each eye at the 1-month follow-up and remained stable throughout the clinical course. Despite this, small areas of metamorphopsia paracentrally worse in the left eye compared with the right eye persisted on Amsler grid testing. Humphrey visual field 10-2 Swedish Interactive Thresholding Algorithm Standard was performed at the 2-month follow-up and confirmed paracentral defects worse in the left eye than in the right eye (Figure 6). At the 3-month follow-up, there was resolution of the retinal whitening and cotton wools spots and near resolution of the paracentral acute middle maculopathy. Optical coherence tomography showed central subfoveal thickness of 262 microns in the right eye (Figure 3E) and 252 microns in the left eye (Figure 4E). There was parafoveal inner nuclear layer thinning worse in the right eye (Figure 3F) compared with the left eye (Figure 4F). En face optical coherence tomography at the level of the mid-retina showed multifocal patchy hyporeflectivity worse in the right eye (Figure 3G) compared with the left eye (Figure 4G), which corresponds to the inner nuclear layer thinning on cross-section. There is also inner retinal thinning in both eyes supertemporal to the fovea (Figures 3H and 4H, right and left eye, respectively) that correspond to the previous areas of internal limiting membrane hyperreflectivity. The superficial capillary plexus on optical coherence tomography angiography was unchanged from the initial presentation in the right eye (Figure 5E) but showed worsening of the abnormal foveal avascular zone with patches of capillary dropout in the left eye (Figure 5G); the deep capillary plexus showed worsening of the multifocal ovoid areas of signal attenuation due to capillary dropout in both eyes (Figure 5F and 5H, right and left eye, respectively).

DISCUSSION
To our knowledge, there are 4 published case reports describing Purtscher retinopathy with paracentral acute middle maculopathy.12–15 Chen et al first reported a case due to a motor vehicle accident and hypothesized paracentral acute middle maculopathy lesions were previously described as Purtscher flecken.12 Tokimitsu et al reported a case with bilateral persistent paracentral scotoma following a car accident 20 years prior; inner retinal layer thinning and capillary loss on the deep capillary plexus was found on optical coherence tomography and optical coherence tomography angiography, respectively.13 Based on these findings, a final diagnosis of paracentral acute middle maculopathy due to Purtscher retinopathy was made.13 Next, Rivera-De Le Parra and Fromow-Guerra reported a case due to tibia and fibula fractures while playing soccer; hyperreflective bands in the inner nuclear layer and deep capillary ischemia were demonstrated on optical coherence tomography and optical coherence tomography angiography, respectively.14 Woo and Vien reported a case with polytrauma following a recent suicide attempt with similar findings to the prior cases.15 In the present case, in addition to these classic findings, there is hyperreflectivity of the internal limiting membrane on optical coherence tomography.
Purtscher retinopathy is a clinical diagnosis based on etiological factors in association with clinical signs.1–3 Patients typically present with sudden painless vision loss of variable severity or bilateral paracentral scotomas, hour to days following the inciting event.1–3 Cotton wool spots are the most common ocular sign followed by retinal hemorrhages.1,2 Although Purtscher flecken is pathognomonic for Purtscher retinopathy, it is only present in approximately 50% of cases.1,2 Purtscher flecken is described as polygonal discrete areas of inner retinal whitening with a 50-micron clear zone between it and the adjacent retinal vessels confined to the posterior pole.1,3 Purtscher flecken is deeper in the retina compared with cotton wool spots.1,12 In fact, Chen et al described Purtscher flecken as ischemia of the intermediate and deep capillary plexus, which is the same as paracentral acute middle maculopathy.12 Patients with Purtscher retinopathy may also present with optic disc edema, but this is rare.2 Bilaterality of clinical signs is present in 60%-75% of cases.1,2
There are multiple theories about the pathogenesis of Purtscher retinopathy but the most likely is an embolic occlusion of the retinal precapillary arterioles.1,2 Potential sources of emboli include air, fat, platelets, fibrin, leukocyte aggregates, and exogenous particles.1,16 Understanding the retinal blood supply explains why the ischemic lesions are concentrated in the posterior pole.16 There are 4 vascular networks in the macula.9,17 The superficial capillary plexus is supplied by the retinal precapillary arterioles and is located in the ganglion cell layer.16,17 There are 2 deeper capillary networks, the intermediate capillary plexus and the deep capillary plexus, located above and below the inner nuclear layer, respectively.17 These 2 deeper plexuses are referred to collectively as the deep vascular complex and are supplied by vertical anastomoses from the superficial vascular plexus.17 Because the precapillary arterioles supply the superficial capillary plexus, which in turn supplies the deeper vascular, occlusion of the precapillary arterioles can result in retinal ischemia throughout the inner retinal layers, as is seen in Purtscher retinopathy. Finally, there is a radial peripapillary capillary plexus that runs parallel to the nerve fiber layer axons.17 This network has fewer arteriole anastomosis, making it susceptible to ischemia.16 Occlusion to these capillaries would result in a peripapillary geographic distribution of Purtscher flecken.16 The demarcated regions separating Purtscher flecken from neighboring retinal arterioles correspond to the capillary-free zone surrounding the arterioles.16
Paracentral acute middle maculopathy presents clinically as bilateral paracentral scotomas.5,6 Fundus examination may be normal or reveal subtle, deep, white or gray parafoveal lesions.6 It is a distinct optical coherence tomography–based entity characterized by hyperreflective band-like lesions primarily involving the inner nuclear layer, with potential extension into the adjacent inner and/or outer plexiform layers.5–7 Paracentral acute middle maculopathy is considered the earliest form of retinal infarction.18 Although paracentral acute middle maculopathy may occur as an isolated clinical entity, it frequently coexists with other retinal pathologies, such as retinal vein or artery occlusions.6,7,10,11 Systemic conditions linked to paracentral acute middle maculopathy include hypertension, diabetes mellitus, sickle cell disease, Purtscher and Purtscher-like retinopathy, and autoimmune disorders.6–8
Paracentral acute middle maculopathy develops from impaired perfusion of the deep retinal vascular complex, specifically the deep capillary plexus and to a lesser extent the intermediate capillary plexus, which is responsible for the blood flow to the middle retina.6,7,18 The deep capillary plexus lacks major arterial supply, so it may maintain a lower perfusion pressure than the superficial capillary plexus.9,18 The oxygen demand of the macula, especially at the level of the inner nuclear layer, outer plexiform layer, and photoreceptor inner segments, is higher than any other region in the retina.6,7,9,12,18,19 Although the choroidal vasculature density is greater in the macula, oxygen diffusion from the choroid is limited by retinal thickness, which is greatest perifoveally.6 Additionally, the density of the capillary system is limited in this same region to optimize high visual resolution.6 This creates a watershed zone in the middle retina that is highly susceptible to ischemia.6,9
Purtscher retinopathy and paracentral acute middle maculopathy can further be investigated with multimodal imaging, such as color fundus photography, optical coherence tomography, optical coherence tomography angiography, and fluorescein angiography.5–7,18,20–22 Optical coherence tomography can be essential in pinpointing the retinal layers affected by ischemia.5–7,18 Acute retinal ischemia leads to edema, which is demonstrated as hyperreflectivity and thickening on optical coherence tomography.23 Cotton wool spots are represented by hyperreflectivity of the nerve fiber layer.6,7 Acute paracentral acute middle maculopathy exhibits perifoveal hyperreflectivity in the inner nuclear layer.5–7 The chronic sequela of paracentral acute middle maculopathy includes localized atrophy of the inner nuclear layer (as seen in this case) (Figures 3F, 4F, and 4H), described as a retinal ischemic perivascular lesion, reflecting underlying ischemic injury to the deep retinal capillary plexus.5,7,8,12 In addition to thinning of the inner nuclear layer, associated outer plexiform layer elevation may occur and present as a characteristic undulating contour in the middle retinal layers, serving as a hallmark for resolved paracentral acute middle maculopathy.
In Purtscher retinopathy, Purtscher flecken is represented by hyperreflectivity of the inner retinal layers.12 Both Purtscher flecken and paracentral acute middle maculopathy represent deep capillary ischemia; however, Purtscher flecken tend to be peripapillary, whereas paracentral acute middle maculopathy lesions are perifoveal.15,24 In addition to cotton wool spots and paracentral acute middle maculopathy lesions, this case revealed hyperreflectivity at the level of the internal limiting membrane that corresponds to inner retinal whitening on fundoscopy. We hypothesize this is due to microocclusion of the superficial capillary plexus located in the ganglion cell layer related to the Purtscher retinopathy; none of the previously published case reports on Purtscher retinopathy have reported this finding.
En face optical coherence tomography of the middle retina can aid in the diagnosis of paracentral acute middle maculopathy.25 Sridhar et al published a case series in which en face optical coherence tomography showed well-demarcated areas of hyperreflectivity in 3 different patterns depending on the etiology: arteriolar, fern-like, and globular.25 In this case, the globular pattern is present (Figures 3C and 4C) with multifocal ovoid patches of the middle retina hyperreflectivity representing distal ischemia in smaller terminal retinal arterioles, precapillaries, or capillaries.25 On follow-up en face optical coherence tomography, the areas of hyperreflectivity resolve and are replaced by variable areas of hyporeflectivity representing middle retinal atrophy (Figures 3G and 4G).25
Unlike traditional fluorescein angiography, in which only the superficial capillary plexus is viewed, optical coherence tomography angiography enables high-resolution, noninvasive visualization of the microvasculature of the superficial retinal capillary plexus, deep retinal capillary plexus, outer retina, and choriocapillaris.13,25 Through optical coherence tomography angiography, vascular density and flow dynamics can be observed.25 For diagnosing Purtscher retinopathy, optical coherence tomography angiography may show areas of capillary dropout in the superficial and/or deep capillary plexus.13 In the early stage of paracentral acute middle maculopathy, there may be normal flow in the deep capillary plexus demonstrated.25 Over time, there is dropout of the deep capillary plexus correlating to the middle retinal atrophy, which is demonstrated on optical coherence tomography angiography as signal attenuation or hyporeflectivity.25 Although partial vascular recovery may occur, the capillary dropout on optical coherence tomography angiography often remains as a marker of prior ischemia.25
The mainstay treatment for both Purtscher retinopathy and paracentral acute middle maculopathy is observation. Isolated case reports suggest that Purtscher retinopathy could be managed with intravenous steroids.3 It is hypothesized that steroids stabilize the membranes of neurons and microvascular channels to prevent ischemia and retinal cell death.22 There is one published systematic review comparing treatment with steroids to no treatment.26 In that review, visual acuity improved regardless of receiving steroids or not, which supports that Purtscher retinopathy is self-limiting.26 For paracentral acute middle maculopathy, the clinical focus of its management is directed toward identifying and addressing underlying systemic or vascular risk factors.6,7
Overall, patients demonstrated a favorable prognosis with Purtscher retinopathy.2 Purtscher flecken, cotton wool spots, and retinal hemorrhages typically resolve after about 1 month.3 No specific clinical features indicate poor visual prognosis, but trauma-related complications may also occur.1,2 The overall prognosis for patients with paracentral acute middle maculopathy is good but can range depending on the severity of initial presentation.14,27 Persistent visual deficits, such as paracentral scotoma, may be experienced as a result of the inner nuclear layer thinning.6
CONCLUSION
Purtscher retinopathy with concurrent paracentral acute middle maculopathy can be induced by underlying retinal vascular occlusions caused by trauma. Given that ischemic events can produce significant ocular symptoms such as blurred vision and paracentral scotomas, along with signs of retinal ischemia, Purtscher retinopathy and paracentral acute middle maculopathy should be considered as differential diagnoses for patients presenting with signs of retinal ischemia. In summary, this case highlights the concurrent presentation of Purtscher retinopathy and paracentral acute middle maculopathy, underscoring the importance of recognizing overlapping clinical features.
TAKE HOME POINTS
-
Purtscher retinopathy and paracentral acute middle maculopathy should be differential diagnoses for patients presenting with sudden decreased vision and paracentral scotomas after trauma.
-
Purtscher flecken is pathognomonic for Purtscher retinopathy but only present in approximately half of cases. The most common ocular sign of Purtscher retinopathy is cotton wool spots.
-
Paracentral acute middle maculopathy may represent the only ocular sign of underlying systemic conditions and warrants urgent stroke work-up cases with an unclear etiology.
-
Observation is the mainstay treatment for both Purtscher retinopathy and paracentral acute middle maculopathy, and no distinct clinical features were found to predict poor visual prognosis for either condition.
DISCLAIMER
The contents of this work do not represent the view of the Department of Veterans Affairs or the United States Government.
No identifiable health information was included in this case report
CONFLICTS OF INTEREST
The authors declare no conflicts of interest.
FUNDING
The authors declare no funding sources.