
INTRODUCTION
Since the early 1960s, intravenous fundus fluorescein angiography (FFA) has been a mainstay in the diagnosis and treatment of vascular abnormalities of the retina and choroid.1 Given the limitations of FFA in examining the choroid, in the late 1980s and early 1990s, indocyanine green angiography became a more widely used adjunctive procedure to view the choroidal vasculature.1 Both FFA and indocyanine green angiography require intravenous injection of dye (sodium fluorescein or indocyanine green), and adverse patient responses are therefore possible.2,3
Thirty-five years or so after the introduction of FFA, retinal imaging again shifted dramatically with the introduction of the first commercial optical coherence tomography (OCT) instrument in 1996.4 The emergence of spectral domain OCT was shortly followed by the commercial introduction of optical coherence tomography angiography (OCTA) in the mid-2010s.4 In OCTA, multiple OCT B-scans at a particular location are performed and compared to detect motion associated with blood flow.4 This allows for differentiation of blood cell movement from static tissue to create a dye-less angiography image.5,6 The first OCTA used spectral domain OCT. Now there are swept-source OCTA models and, fairly recently, widefield swept-source OCTA, which allow for a 24 × 20-mm image size.7,8
The indications for FFA have declined with the introduction of OCT and OCTA.9–11 With a decade of experience with OCTA, how is the use of OCTA fitting into the retinal imaging landscape? Does OCTA have the potential to limit the use of dye-based imaging tests to only a small group of clinical situations? No identifiable health information was included in this paper.
POINT (DR. BEDWELL): OCTA CAN BE USED AS A STANDALONE IMAGING MODALITY IN PLACE OF FUNDUS FLUORESCEIN ANGIOGRAPHY IN MOST CLINICAL SCENARIOS
Although FFA will continue to play a role in retinal imaging, there are many clinical scenarios in which OCTA can replace FFA. The key areas to make that assessment revolve around the comparison of safety, performance, and clinical utilization.
Safety Profile
The most striking advantage that OCTA holds over FFA is the noninvasive safety profile. OCTA is a zero-risk test. Even though dye-based angiography is viewed as a safe procedure, it is not risk free. The Fluorescein Angiography Complication Survey assessed FFA-associated adverse events and found a rate of 1:63 for moderate adverse events such as urticaria and syncope, and 1:1900 for severe adverse events, falling into either cardiopulmonary or neurologic.12 The Fluorescein Angiography Complication Survey estimated the risk of death from FFA at 1:220 000.12 These serious events are rare, but patients undergoing FFA can commonly encounter nuisance complications, categorized as mild, self-limiting adverse events. In a prospective study of 1500 individuals undergoing FFA, 6.83% experienced nausea, 1.35% vomiting, 1.06% urticaria, 0.38% bronchospasm, and 0.01% laryngeal edema.13 By comparison, indocyanine green angiography has a slightly safer profile than FFA. A study of 1923 indocyanine green videoangiographies revealed 3 (0.15%) cases with mild adverse reactions, 4 (0.2%) cases of moderate adverse reactions, and 1 case (0.05%) of a severe adverse reaction.3 In this latter study, there were no deaths. Severe reactions with indocyanine green angiography, although rare, were also reported in another study that included more than 3700 indocyanine green angiography procedures (hypotension occurred in 0.05%),14 and in 2 published case reports.15,16

Acquisition Speed and Efficiency
OCTA further surpasses FFA in acquisition speed and efficiency. Depending on the scan parameter, most OCTA images can be acquired in a matter of minutes by a single technician. On the other hand, FFA necessitates a photographer and the appropriately trained medical staff to inject the intravenous dye. The procedure, including obtaining the imaging sequence, takes 10 to 20 minutes.17–19 The ease of OCTA makes it ideal for many optometric practice settings.
Similar to the introduction of OCT, there is a learning curve to interpret OCTA and tease out the reliable data from artifacts.20 It is reminiscent of the early years using OCT, when practitioners relied heavily on the color-coded sector maps, that in turn led to many false positive “red disease” diagnoses of glaucoma. Interpreting OCTA relies heavily on an understanding of the retinal and choroidal vasculature. Fortunately, as of January 1st this year, the efforts of learning OCTA are now properly recognized and reimbursed, albeit at a lower rate than FFA, under Current Procedural Terminology code 92137.
A single OCTA image offers 3-dimensional viewing of retinal and choroidal circulation, whereas the images obtained during FFA are all 2-dimensional and isolated to the superficial retinal circulation.6 Within the retinal vasculature, OCTA can tease out the capillary plexi, differentiating the superficial, intermediate, and deep capillary networks. Quantitative assessments can be made such as measuring the foveal avascular zone and vessel density.6 Hyperpermeable vessels, occurring with macular edema or a leaking choroidal neovascular membrane, do not alter OCTA images as occurs in FFA. Even in the presence of macular edema, capillary perfusion can still be appreciated on OCTA.6
OCTA: Clinical Benefits
Aside from safety and convenience, how is OCTA clinically useful? The most clinically practical applications, particularly within optometry, include diabetic vascular assessment and monitoring conditions at risk for macular neovascularization.
For diabetic retinopathy, some OCTA models provide quantitative assessments such as foveal avascular zone size, vessel density, and perfusion density. The accuracy in measuring the foveal avascular zone with FFA is less than that of OCTA, and vessel density and perfusion density cannot be quantified with FFA.5,6,21,22 With increasing severity of diabetic retinopathy, the foveal avascular zone increases in size and the foveal avascular zone shape loses circularity.22,23 Similarly, in the superficial capillary plexus, the vessel density and perfusion density decrease in correlation with increasing diabetic retinopathy severity.22 OCTA can detect preclinical retinopathy, particularly small microaneurysms (<30 microns), as long as there is sufficient flow or movement through them.24 OCTA is criticized for being inferior to FFA in detection of microaneurysms.25,26 But as the necessity for focal laser treatment has declined in the era of anti–vascular endothelial growth factor, this downside to OCTA is now less clinically meaningful.
Additionally, OCTA can uncover and quantify capillary nonperfusion or ischemia seen as areas void of vasculature in the capillary plexi. This has applications beyond diabetic retinopathy, such as in venous and arterial occlusions. Current evidence shows that OCTA is similar to FFA in detecting nonperfusion.26,27 Additionally, OCTA, particularly widefield OCTA, is non-inferior to FFA in detection of proliferative disease.7,26–29 Cui and colleagues compared ultra-widefield color photography, widefield swept-source OCTA, and ultra-widefield FA in 152 eyes.7 They found widefield swept-source OCTA and ultra-widefield FA were comparable in detection rate of microaneurysms, intraretinal microvascular abnormalities, neovascularization elsewhere and neovascularization of the disc, and areas of nonperfusion.7 Cui and colleagues suggested the combination of widefield OCTA and ultra-widefield color photography may be a reasonable “alternative” to fluorescein angiography.7 Widefield OCTA does not reach the same peripheral viewing extent as ultra-widefield FA. Despite that, Russell and colleagues demonstrated by overlaying widefield swept-source OCTA over an ultra-widefield FA image of eyes with proliferative diabetic retinopathy that 98.3% of neovascularization elsewhere/neovascularization of the disc lesions were detectable.29
Case: OCTA Use in Proliferative Diabetic Retinopathy
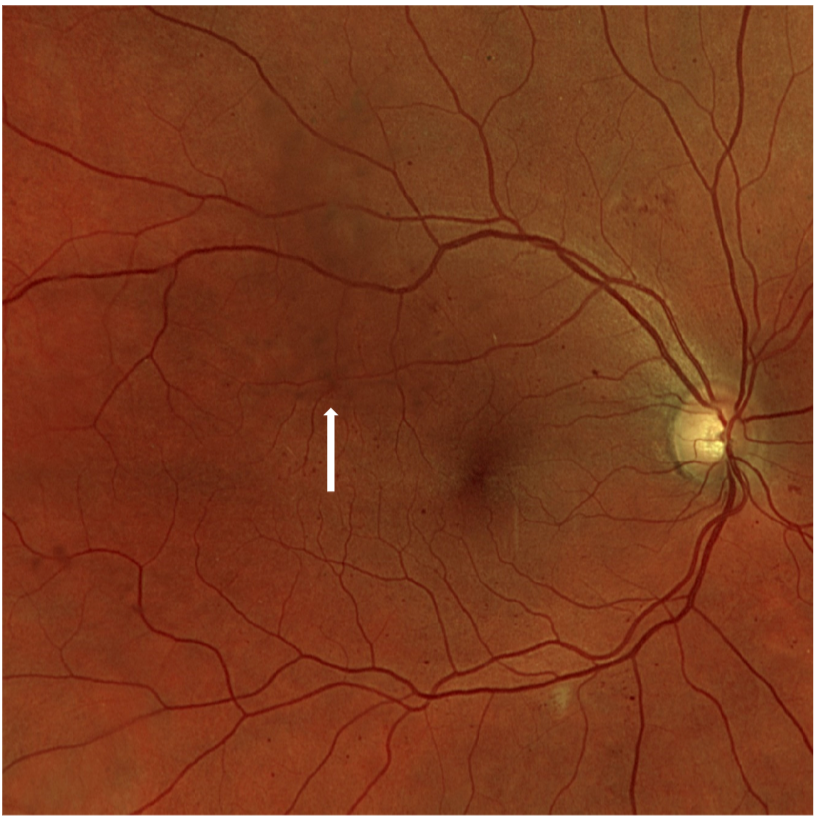
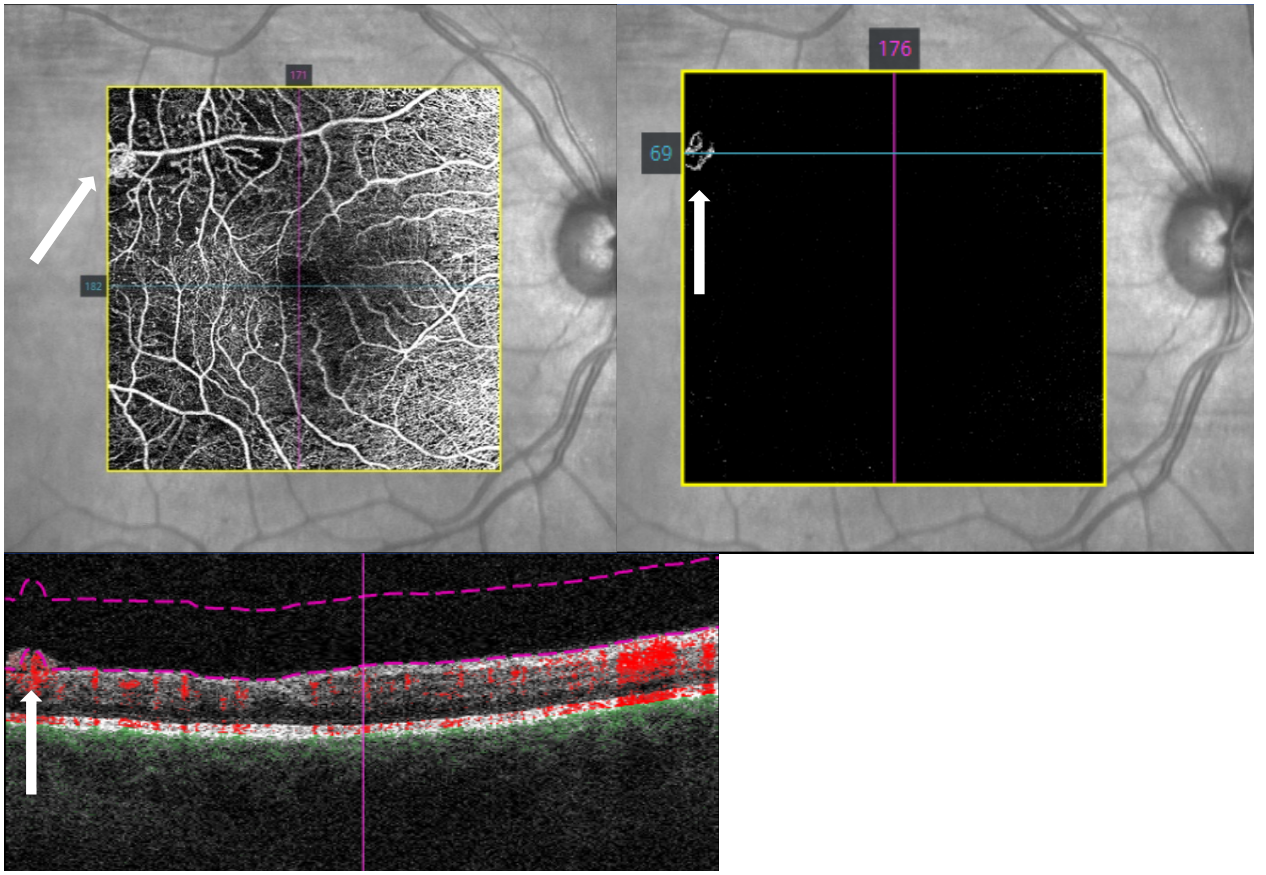
The following case shows a patient with diabetic retinopathy that developed subtle neovascularization elsewhere adjacent to an area of capillary nonperfusion. The neovascular frond is poorly distinguished in the color photograph (Figure 1). OCTA (Figure 2) clearly shows a neovascular network breaching the vitreoretinal interface, distinguishing this as neovascularization elsewhere as compared to intraretinal microvascular abnormalities. The patient was referred to retinal ophthalmology and subsequently treated with panretinal photocoagulation without the necessity of dye angiography.

_images_demonstrate_the_developme.png)
Case History and Findings
-
57-year-old White female
-
Presented for monitoring of severe nonproliferative diabetic retinopathy in both eyes
-
Type 2 diabetes mellitus × 15 years, most recent hemoglobin A1C 10.6%, hypertension, hyperlipidemia
-
Best-corrected visual acuity 20/20 in each eye
-
Fundus examination showed intraretinal hemorrhages in all 4 quadrants in each eye, no diabetic macular edema in either eye.
-
OCTA revealed new subtle frond of neovascularization elsewhere adjacent to macular capillary nonperfusion in the right eye indicating progression to proliferative diabetic retinopathy.
OCTA also demonstrates advantages in the setting of macular neovascularization. This is most evident in monitoring age-related macular degeneration but also can be applicable in any condition at risk of choroidal neovascularization such as high myopia, macular dystrophy, central serous chorioretinopathy, ocular histoplasmosis syndrome, and other macular disorders. In 2018, researchers recognized the capability of OCTA to detect subclinical, nonexudative macular neovascularization.30 This entity represents a neovascular network that lacks findings of exudation, lacks fluid on OCT, and does not leak on FFA.30,31 Over a 2-year follow-up, intermediate age-related macular degeneration eyes with nonexudative macular neovascularization are 13.6 times more likely to progress to the exudative form as compared with intermediate age-related macular degeneration eyes without.31 The timespan for progression from nonexudative to exudative macular neovascularization is still unclear, ranging in cases from months to years and as such treatment is not recommended for nonexudative macular neovascularization. But here OCTA offers an opportunity that FA does not, to better recognize a precursor to advanced age-related macular degeneration development and monitor accordingly.
COUNTERPOINT (DR. FOGT): OCTA CAN ONLY REPLACE FUNDUS FLUORESCEIN ANGIOGRAPHY IN SELECT CLINICAL SCENARIOS AND ONLY WHEN PRACTITIONERS HAVE SUFFICIENT EXPERIENCE IN INTERPRETING OCTA IMAGES AND IN CORRECTING OCTA ARTIFACTS SUCH AS SEGMENTATION ERRORS
FFA has been used for more than 60 years to evaluate the retinal vasculature and to some extent the choroidal vasculature.1 After intravenous injection of sodium fluorescein, the dye travels through the circulation to the eye. When the fluorescein is stimulated by blue light, it emits green light, so the camera used in FFA contains a blue (exciter) filter and a green (barrier or collector) filter. Photographs of the posterior segment are taken rapidly (every 1-2 seconds) at first and then less often in a tapered manner over 10 to 20 minutes.17–19 In the presence of disorders that compromise the retinal vasculature such as diabetic retinopathy or retinal vasculitis, leakage of fluorescein into the retinal tissues may occur.1 In addition, fluorescein leakage may occur from retinal or choroidal neovascularization. Indocyanine green angiography is another dye-based procedure. Indocyanine green is particularly useful in viewing abnormal choroidal vasculature such as choroidal neovascularization because it absorbs and emits near-infrared wavelength light.1 Near-infrared light more readily penetrates through pigment including that of the retinal pigment epithelium, and indocyanine green does not leak as readily from the choriocapillaris compared with sodium fluorescein.1 Indocyanine green angiography thereby results in a better view of the choroidal vasculature compared with FFA.
Clinical Utility of OCTA Versus Dye-Based Angiography in Retinal and Choroidal Disease
As pointed out above, the primary problems with dye-based assessments of the retinal vasculature including FFA and indocyanine green angiography are the potential of adverse events and the time required to complete the test. Adverse reactions such as nausea and vomiting and in rare instances severe anaphylactic responses can occur with dye-based tests, and these reactions can of course be avoided with noninvasive OCTA testing. In a recent paper, Kornblau and El-Annan reviewed the literature on adverse reactions associated with FFA.2 This paper included some of those papers mentioned previously in the reference list.12,13,15,16 The reported incidence of mild adverse reactions was 1.24% to 17.65%, of moderate reactions was 0.2% to 6%, and of severe reactions was 0.04% to 0.59%. There were 1:100 000 to 1:220 000 deaths.2 FFA is contraindicated in pregnancy and in patients with a history of severe allergic reaction to fluorescein.17 Caution must be exercised when performing FFA in patients with renal disease or cardiovascular disease, although these disorders do not necessarily preclude the procedure from being performed.17 The time required to complete FFA may be 10 to 20 minutes, compared with 5 minutes or less for OCTA testing. Further, recent studies demonstrate that OCTA is at least comparable to FFA (i.e., not inferior) in identifying vascular lesions or conditions such as intraretinal microvascular abnormalities, retinal neovascularization, choroidal neovascularization, areas of retinal nonperfusion, and pachychoroid neovasculopathy.32–35 OCTA probably also allows practitioners to quantify changes in the foveal avascular zone more easily compared with FFA.36
Despite the potential problems associated with FFA and indocyanine green angiography and the non-inferior or even superior findings of traditional B-scan OCT and OCTA over these dye-based tests for detection and assessment of many vascular lesions,37,38 a 2023 survey of practicing Australian optometrists administered by Cheung and colleagues revealed that these practitioners were “neutral” (3.4 on a 5 point Likert scale) regarding the usefulness of OCTA for daily [clinical] practice.39 Practitioners reported that OCTA was “less enjoyable to use and less endorsed by peers”, and that they were not as confident in interpreting OCTA images compared to OCT, color fundus imaging, ultra-widefield imaging, and fundus autofluorescence.39 The authors did not ask practitioners to compare the usefulness of OCTA to FFA. Whether the respondents’ attitudes toward OCTA were in part driven by the idea that the usefulness of OCTA is limited because FFA is at least comparable to OCTA, or the idea that FFA results are more easily interpreted compared with results from OCTA, is not known. What is evident from this study is that there are factors limiting the perceived clinical usefulness of OCTA in this cohort.
Artifacts of OCTA Images and Implications for Interpretation
There are some limitations of OCTA that might account for the lower-than-expected practitioner rating of the usefulness of this device reported by Cheung and colleagues.39 One major issue with OCTA is the problem of artifacts associated with the OCTA images. Extensive attempts to remove or reduce these artifacts have occurred in recent years, but skilled experience on the part of the provider is still required to account for them.40–42 In a study from 2020 by Holmen and colleagues, at least 1 artifact was seen in 97.3% of images of OCTA images (406 images analyzed).43 So-called signal artifacts can lead either to the appearance of blood flow when none is present or can lead to apparent lack of blood flow when flow is present.44,45 For example, an obstruction in the vitreous or in the more superficial retinal layers could cast a shadow in the deeper layers (shadow artifact). Another signal artifact, termed the motion artifact, is associated with eye movements of the patient during the multiple scans required to obtain the OCTA image.46 Motion artifacts could induce apparent flow when none is present. The presence of motion artifacts suggests that OCTA images may be difficult to interpret when obtained from patients with less reliable fixation or from patients with disorders affecting fixation such as poor vision or eye movement abnormalities.47 Avoidance of motion artifacts may require that the OCTA operator strongly encourage the patient to maintain stable fixation when possible and to minimize blinks. Several seconds of steady fixation is required to obtain good OCTA images, whereas a reasonable single fluorescein image can be obtained in much less time.
Still other artifacts in OCTA images include segmentation artifacts, in which the boundary of a retinal layer or slab is mischaracterized, and projection artifacts whereby vasculature in superficial tissue layers appears to be in deeper layers.20,48 Segmentation artifacts can likely be accounted for by manual segmentation, but this requires provider expertise and adds time to the processing and interpretation of OCTA images.45
All of this suggests that proper interpretation of OCTA images requires experience on the part of the practitioner. In one article, it was suggested that a “four-up” review of images be employed for this purpose.20 In this method, the practitioner looks at the en face slab(s) of the OCTA images, the en face (coronal) structural OCT image, the “traditional” structural OCT cross-section (B-scan), and the vascular flow overlay. Learning to combine the information from all of these scans would likely require significant experience, and to gain this experience, a practitioner would require a patient population that regularly presents with ocular diseases such as diabetic retinopathy, age-related macular degeneration, and glaucoma.49 Although experience is certainly necessary to accurately interpret fluorescein angiograms, since FFA has been used for many decades, the nuances involved in analyzing fundus fluorescein angiograms are likely better established when compared with the rapidly evolving science of OCTA interpretation.50
Limitations of OCTA in Demonstrating Vascular Leakage, Pooling, and Staining
Another limitation of OCTA is that, unlike FFA, OCTA cannot demonstrate vascular leakage, pooling of fluorescein (i.e., increased intensity of the fluorescence over time but no increase in the area of fluorescence), or staining of tissues (leading to late hyperfluorescence). FFA can indicate both the presence of vascular leakage and the rate at which this leakage occurs. These findings not only can be useful in assessing the source of the leakage but also may be helpful in determining the likely underlying cause of the leakage.51 For example, in cases of central retinal artery occlusion, OCTA can reveal areas of capillary nonperfusion in both the superficial capillary plexus and deep capillary plexus as well as changes in the circularity of the foveal avascular zone.52 However, FFA is considered essential in eyes with central retinal artery occlusion, as it reveals the extent of the remaining vascular perfusion,53 and it indicates when a vascular workup for an arteritic condition that may have led to the occlusion is necessary.54 These advantages of FFA over OCTA are perhaps not as strong as they first appear. Leakage of dye in more superficial tissue layers on FFA may block visualization of leakage from deeper tissues or block areas of interrupted blood flow or ischemia, and cross-sectional OCT allows for vascular leakage to be inferred by demonstrating retinal pigment epithelial or retinal detachments resulting from fluid leakage into areas including the sub–retinal pigment epithelium space, the subretinal space, and the neurosensory retina. In addition, artificial intelligence has been applied to OCTA images to infer vascular leakage and vascular occlusion.55
Nevertheless, FFA remains an important qualitative method to help in detecting the source and the rate of vascular leakage, as well as the extent of reduced vascular filling. Recently, the panretinal leakage index as assessed with ultra-widefield fluorescein angiography has been shown to correlate with diabetic retinopathy severity.56 The panretinal leakage index is calculated as the percentage of an area of interest that shows vascular leakage. Further, in a 2022 paper by Invernizzi and colleagues in which experts were asked to give opinions on the utility of FFA versus OCTA for the management of uveitis, while a number of positive features of OCTA were described, it was pointed out that detection of peripheral vascular leakage with ultra-widefield fluorescein angiography is critically important in determining the treatment of uveitis.57
Limitations of OCTA in Imaging Slow Vascular Flow Velocity
Yet another limitation of OCTA is the ability to detect lesions or retinal areas that manifest slow vascular flow velocity. In some studies, fewer microaneurysms have been detected on OCTA compared with FFA in cases of diabetic retinopathy.25,26 This is not the case in every study.58 Assessment of the deep retinal capillary plexus using OCTA may identify more microaneurysms compared with FFA.58 If FFA allows for detection of more microaneurysms compared with OCTA, the question that arises is whether this difference in detection rate is actually of clinical benefit. For example, typical B-scan OCT images are likely to demonstrate fluid secondary to leakage from microaneurysms, and OCT may therefore reduce the need to detect vascular leakage from microaneurysms directly with FFA. Once macular edema is detected and it is determined that treatment is required, first-line treatments for this condition usually involve intravitreal injections of anti–vascular endothelial growth factor medications. Unlike laser photocoagulation, treatment of macular edema with intravitreal anti–vascular endothelial growth factor medications may not require careful localization of microaneurysms. However, multiple anti–vascular endothelial growth factor injections are likely to be required, and this then places potential burdens on the patient related to money, time, and transportation. Laser photocoagulation, perhaps in conjunction with anti–vascular endothelial growth factor medications, might therefore be used in treating a patient’s macular edema from leaking microaneurysms.59,60 In those cases, identification of microaneurysms, which might be better with FFA compared with OCTA, is likely to be important in guiding laser procedures.
Potential Limitations of the Field of View of OCTA
A final limitation of OCTA imaging compared with FFA is the relatively limited field of view of OCTA images. This has taken on added significance, as it has been shown that ultra-widefield fluorescein angiography can help in identifying predominately peripheral lesions, which are useful in predicting progression of nonproliferative diabetic retinopathy.61 The recent development of swept-source OCTA technology has allowed for montages of OCTA images of 15 × 15 mm (56°) and even 24 × 20 mm (120°), which are well below the angular retinal area encompassed by ultra-widefield fluorescein angiography (200°) but much larger than the 3 × 3-mm and 6 × 6-mm images employed until recently in OCT angiography.7,62 Interestingly, although increasing the field of view of OCTA images probably lowers the resolution of these images, in a study comparing widefield (15 × 15 mm) swept-source OCTA to ultra-widefield fluorescein angiography, microaneurysms, intraretinal microvascular abnormalities, neovascularization elsewhere, neovascularization of the disc, and areas of nonperfusion in diabetic retinopathy were detected equally well by these 2 methods.7 Similar results were reported in a study comparing 24 × 20-mm OCTA images to results from ultra-widefield fluorescein angiography (although fewer microaneurysms were noted with OCTA compared with FFA), but in this latter study, the comparison of OCTA images was made only for the superficial capillary plexus and the fluorescein angiography images were scaled to 24 × 20 mm.26 It is unclear how these widefield OCTA results can be reconciled with the finding that peripheral retinal lesions have been shown to be predictive of diabetic retinopathy progression, as it would appear that current OCTA systems cannot image these far peripheral changes. Further study will be needed to determine whether widefield OCTA imaging is as effective in detecting and staging vascular changes in diabetes and perhaps other disorders of the retinal vasculature compared with ultra-widefield fluorescein angiography.63,64
Other Issues That May Encourage or Limit the Use of OCTA
There are other factors that might determine whether practitioners find more value in OCTA than that provided by FFA. For example, because OCTA is a relatively new and rapidly developing technology compared with FFA, at the moment, practitioners may be better able to interpret fluorescein angiograms based on experience.50 The comfort level in interpreting FFA versus interpreting OCTA images may relate to the length of time a practitioner has been in the field. Younger practitioners who have been exposed to OCTA throughout their training and early career may be as well-versed in interpreting OCTA images as they are in interpreting fluorescein angiography images.57
In addition, although OCTA metrics such as vessel density and the size of the foveal avascular zone can be well-quantified, to make efficient use of these metrics, there remains a need to develop standardized classification or grading schemes based on OCTA findings for disorders such as diabetic retinopathy.65,66 Only then can the findings from OCTA be translated into practice protocols.
SUMMARY
OCTA has some clear benefits over dye-based angiography for clinical practice, and these benefits become more apparent as practitioners gain experience in interpreting OCTA images. The rapid development of widefield OCTA platforms also supports these benefits. Examples of the benefits of OCTA are as follows. OCTA may allow the practitioner to noninvasively detect neovascularization at the vitreoretinal interface that may not have been detected with a typical funduscopic examination, or to differentiate this neovascularization from intraretinal microvascular abnormalities. OCTA can also help in identifying the presence or absence of neovascularization in pachychoroid disease, and OCTA is definitely of benefit in detecting and managing nonexudative macular neovascularization. All of these benefits are offered without the invasive need for intravenous dye. However, the inability of current OCTA systems to detect vascular leakage, the inconsistencies of OCTA systems in detecting retinal abnormalities with slow flow, the reduced field of view of OCTA compared with ultra-widefield fluorescein angiography, and the lack of standardization in the grading of disease levels from OCTA images suggests that at least for now, FFA remains the gold standard in diagnosing, staging, and managing retinal disease. As studies of OCTA continue, it is expected that we will gain a better understanding of the extent to which the limitations of OCTA affect its diagnostic capabilities, the extent to which the artifacts associated with OCTA must be accounted for to obtain the most accurate diagnoses, and the extent to which OCTA can complement and perhaps replace FFA.67
DISCLOSURE
Dr. Bedwell has served as a paid advisor for Regeneron.