



INTRODUCTION
Vogt-Koyanagi-Harada disease is a T cell–mediated autoimmune disorder affecting melanocytes, melanin, and retinal pigment epithelium.1 This condition often results in bilateral granulomatous panuveitis with extraocular symptoms such as headache, meningism, alopecia, vitiligo, and tinnitus.2 Although the median age of onset reported in literature varies, the disease is less common in children and older individuals and predominantly affects individuals aged between 20 and 50 years.3 Vogt-Koyanagi-Harada disease also exhibits a female predominance, with rates ranging from 50% to 75%.4 The condition is diagnosed more frequently among certain pigmented populations, particularly Asians, Hispanics, and Native Americans, yet significant geographic and ethnic variability has been observed.3,5
The initial onset of the ocular disease manifests as bilateral granulomatous choroiditis, leading to serous retinal detachment along with optic disc edema and hyperemia. Without adequate treatment, inflammation progresses to involve the anterior segment and eventually leads to recurrent granulomatous anterior uveitis, which can become chronic. This stage is characterized by chorioretinal atrophy and a “sunset glow fundus.”2 The differential diagnosis is broad and includes sympathetic ophthalmia, central serous chorioretinopathy following steroid use, and exudative detachment from malignant hypertension.6,7 Uveal lymphoid infiltration, intraocular lymphoma, uveal effusion syndrome, sarcoidosis, lupus choroidopathy, posterior scleritis, acute posterior multifocal placoid pigment epitheliopathy, acute leukemia, and metastatic carcinoma should also be considered.7,8 Infectious causes of uveitis such as Lyme disease, cat scratch disease, tuberculosis, and syphilis should be ruled out.8–11 This case illustrates the clinical manifestations and treatment of panuveitis associated with Vogt-Koyanagi-Harada disease in a postpartum female. No identifiable health information was included in this case report.
CASE REPORT
A 36-year-old Hispanic woman presented to a community eye clinic with progressively worsening headache, bilateral ocular pain, photophobia, and reduced vision for 2 weeks. She had been diagnosed with migraine headaches and allergic conjunctivitis by an emergency room physician. She was taking over-the-counter pain relievers and olopatadine hydrochloride ophthalmic solution 0.2% (Pataday, Alcon) once daily in both eyes. Her medical history was positive for an uncomplicated labor and delivery 3 months prior, and she was actively breastfeeding.
Snellen visual acuity was 20/200 (pinhole acuity was 20/125) in the right eye and 20/30 with no pinhole improvement in the left eye. Extraocular motilities and confrontation fields were full. Pupil testing was difficult due to the patient’s extreme photophobia, but pupils appeared round and reactive to light with no evidence of an afferent pupillary defect. Slit lamp evaluation revealed periorbital lid edema on the right eye and watery discharge in both eyes. There was 3+ diffuse injection of the bulbar conjunctiva in both eyes. The corneas were clear, with no signs of keratic precipitates. An inferior posterior iris synechia was noted in the right eye. The anterior chambers demonstrated 3+ cells in the right eye and 2+ cells in the left eye. Intraocular pressures measured 9 mm Hg in the right eye and 8 mm Hg in the left eye. Diffuse pigment was noted on the anterior lens capsule of the right eye. A dilated fundus examination was performed. Trace cells were noted in the anterior vitreous of the right eye. The optic discs were pink with distinct disc margins in both eyes. The cup-to-disc ratios were 0.25 round in the right and left eye. Multiple serous retinal detachments were noted in both eyes. No hemorrhages, exudates, or cotton wool spots were observed. The patient was diagnosed with bilateral panuveitis, and treatment was initiated with atropine once a day and difluprednate ophthalmic emulsion 0.05% (Durezol, Novartis) hourly in both eyes. The patient was referred to the retina clinic in 1 day for further evaluation and imaging.
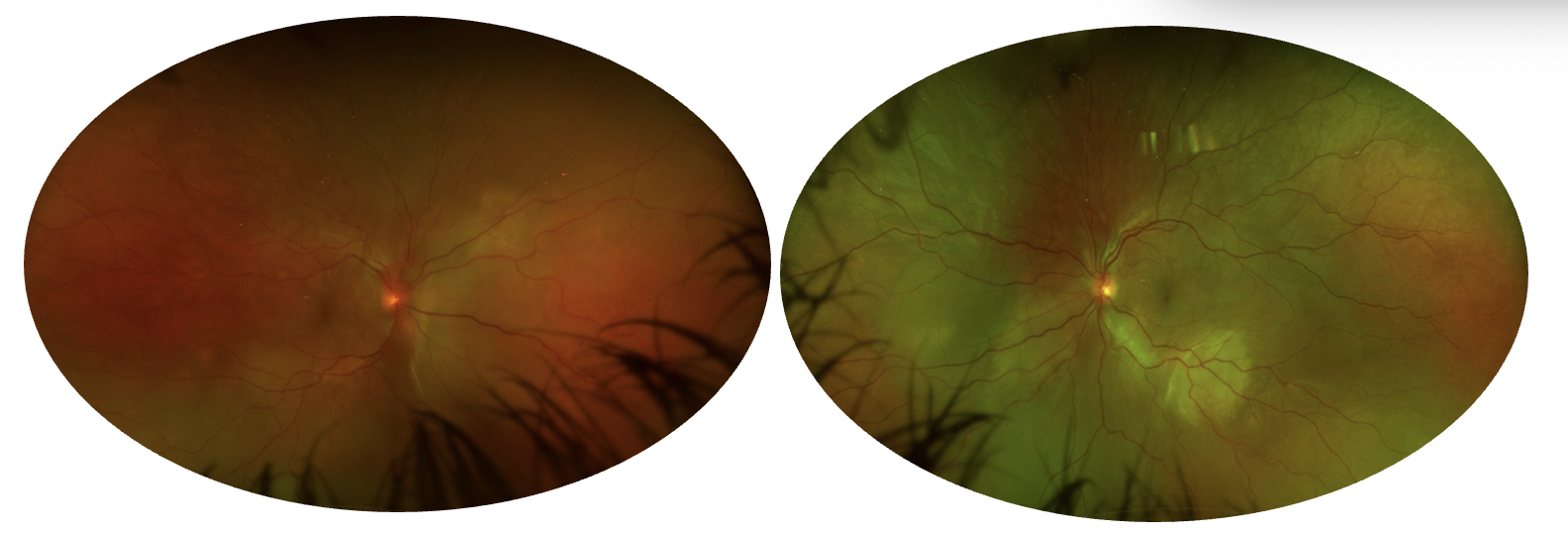
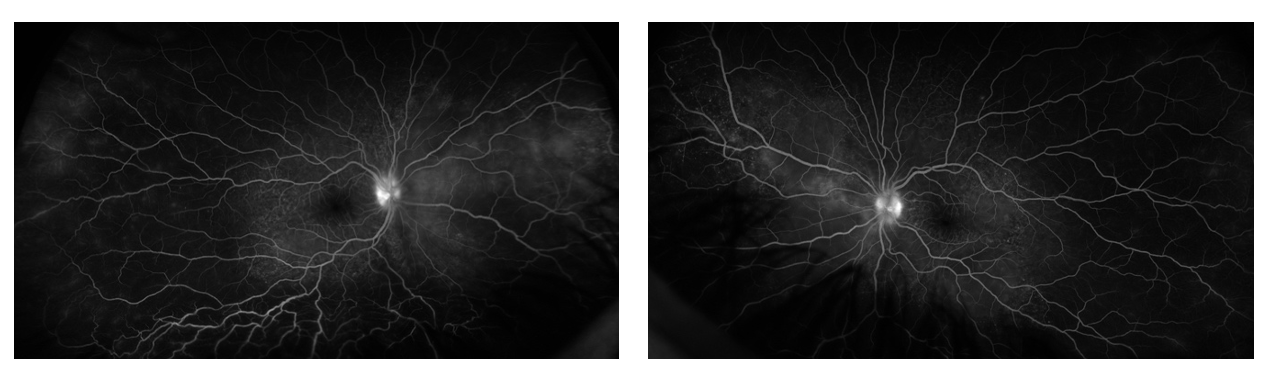
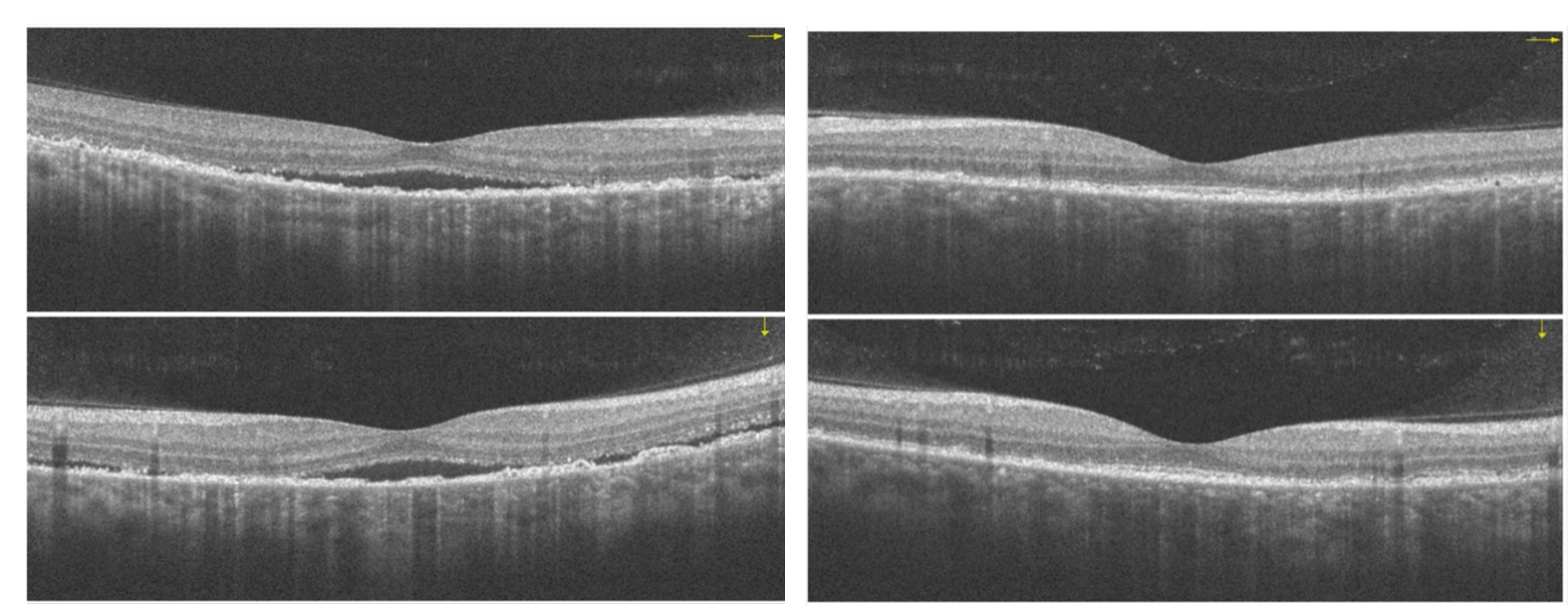
The patient presented to the retina clinic the following day, reporting an improvement in pain and photophobia but worsening vision since starting topical treatment. Snellen visual acuity was reduced to 20/300 (pinhole acuity of 20/100) in the right eye and 20/300 with no pinhole improvement in the left eye. Fundus photography and optical coherence tomography revealed areas of serous retinal detachments and chorioretinal folds in both eyes (Figures 1 and 2). Fluorescein angiography revealed multiple punctate hyperfluorescent foci throughout the macular region and staining of the optic nerve without leakage (Figure 3). There was neither retinal ischemia nor evidence of any other vascular disease patterns. The following laboratory testing was ordered: complete blood count with differential, lipid panel, metabolic panel, urine analysis, thyroid stimulating hormone, hemoglobin A1c, rheumatoid factor, HLA-B27, antinuclear antibody, toxoplasmosis immunoglobulin G, human immunodeficiency virus, rapid plasma reagin, and fluorescent treponemal antibody-absorption test for syphilis, and QuantiFERON for tuberculosis. The results were unremarkable, apart from positive antinuclear antibody.
_and_left_eye_(right)_at_initial_presentation_de.png)
_and_left_macula_(right)_at_initial.png)
_and_left_eye_(right)_demonstrating_punctat.png)
A diagnosis of early-stage Vogt-Koyanagi-Harada disease was made based on the patient’s clinical presentation, which included headache, bilateral panuveitis, serous retinal detachment, and no history of penetrating trauma or ocular surgery prior to disease onset. The findings from optical coherence tomography and fluorescein angiography, along with the exclusion of infectious causes such as syphilis, tuberculosis, and toxoplasmosis, supported a noninfectious etiology consistent with Vogt-Koyanagi-Harada disease. The patient reported no respiratory symptoms or dermatological changes, and the absence of periphlebitis and “candle wax drippings” ruled out sarcoidosis.12 Our diagnosis was supported by the 2021 Standardization of Uveitis Nomenclature Working Group Vogt-Koyanagi-Harada classification criteria for early-stage Vogt-Koyanagi-Harada disease.3 Although additional imaging, such as magnetic resonance imaging and chest x-ray, was considered to facilitate diagnosis, it was not pursued because of the patient being uninsured and unable to undergo the tests because of financial constraints. Treatment was adjusted to add prednisone 80 mg per day and omeprazole 20 mg per day orally in addition to atropine once a day and Durezol hourly in both eyes. The patient’s primary care physician was consulted on the findings, and she was advised to discontinue breastfeeding.
The patient presented for 6 follow-up visits over the course of 1 month after the initial presentation, during which the symptoms and signs gradually improved. Atropine was discontinued on day 15, Durezol dosage was gradually reduced to twice daily, and prednisone dosage was maintained at 80 mg per day orally. On day 30, prednisone dosage was reduced to 70 mg per day orally. At the 59-day follow-up visit, the patient reported that she had reduced her prednisone dosage to 40 mg per day orally based on the advice of her primary care physician because she was experiencing muscle and join pain. At this visit, the Snellen visual acuity was 20/50 (pinhole acuity was 20/25) in the right eye and 20/25 in the left eye. Optical coherence tomography images revealed a significant improvement in macular detachment in the right eye and complete resolution in the left eye (Figure 4). Given the improvement in her signs and symptoms, we recommended that she continue the current dosage until her next follow-up visit in 1 month and our treatment plan was communicated to her primary care physician. Eighty-eight days after the initial presentation, the patient presented to the clinic, reporting extreme blurry vision, pain, and photophobia. She reported that she had discontinued prednisone 10 days prior, following the advice of her primary care physician, despite our recommendation to maintain a dosage of no less than 40 mg per day. Her visual acuities were hand motion at 6 feet in the right and left eye. An exacerbation of the Vogt-Koyanagi-Harada disease was found in both eyes. Treatment was reinitiated, and the patient was referred to a rheumatologist for long-term management of her systemic autoimmune condition. Unfortunately, the patient was lost to follow-up after establishing care with rheumatology.
_and_left_macula_(right)_showing_ne.png)

DISCUSSION
Undertaking the management of noninfectious uveitis can be a challenging task. If we add pregnancy or breastfeeding to the patient profile, management decisions become more complex as they must carefully balance the health and safety of both the mother and the baby. The risk of developing autoimmune disease is significantly elevated during the first year postpartum but tends to decrease thereafter.13 Khashan et al reported an association between pregnancy and the risk of developing maternal autoimmune diseases, with a higher risk observed following cesarean section and a lower risk following abortion.14 Theories suggest that fetal microchimerism, where small amounts of fetal cells persist in the mother, may play a role in the development of autoimmune disease in the postpartum period.15–17
In women with a history of noninfectious uveitis, studies have shown that disease activity is often decreased during pregnancy. However, many experience an increase in uveitis activity within 6 months postpartum.18,19 Similarly, women with Vogt-Koyanagi-Harada disease tend to see improvement in ophthalmic symptoms during pregnancy, followed by exacerbations after delivery.20,21 During pregnancy, the production of endogenous corticosteroids, particularly cortisol, increases significantly.22 In addition, high estrogen and progesterone hormone levels lead to a shift from type 1 T helper cell–mediated cellular immunity to type 2 T helper cell–mediated humoral immunity.23 This shift reduces the production of proinflammatory cytokines, partially suppressing the woman’s immune system, and likely helps to prevent her body from rejecting the fetus. After delivery, endogenous corticosteroid production by the placenta ceases, which may promote reactivation of both humoral and cellular immunity. Furthermore, breastfeeding has been associated with a shift in immune function. A surge in the proinflammatory hormone prolactin occurs with breastfeeding, which has been shown to stimulate the immune response and promote autoimmunity by increasing the production of immunoglobulins, cytokines, and autoantibodies.24 As Vogt-Koyanagi-Harada disease is a T cell–mediated autoimmune disorder, these sudden hormonal shifts can potentially trigger onset or flares of Vogt-Koyanagi-Harada disease in genetically predisposed women.23,25
The link between uveitis, pregnancy, and the postpartum period presents a therapeutic challenge for clinicians, as it necessitates the use of medications that may carry undesirable side effects for the mother and the baby. Although some reports have noted that cases of acute Vogt-Koyanagi-Harada disease at initial onset were effectively managed with either topical corticosteroids or observation alone,26,27 systemic corticosteroids are generally considered the first line of treatment to manage inflammation in Vogt-Koyanagi-Harada disease.28 Periocular steroid injections and local options such as dexamethasone intravitreal implant 0.7 mg (Ozurdex, AbbVie) and fluocinolone acetonide intravitreal implant 0.18 mg (Yutiq, Alimera Sciences) can also be considered.29 Nonfluorinated glucocorticoids, such as prednisone, prednisolone, hydrocortisone, methylprednisone, and methylprednisolone, particularly at low doses, are suitable for use during pregnancy and breastfeeding.30 However, there is 1 reported case of fetal death following intravenous administration of high-dose prednisolone therapy in a pregnant woman with Vogt-Koyanagi-Harada disease, although the exact cause of death was not determined.31 Nursing mothers can take prednisone, but if the dosage exceeds 20 mg per day, it is recommended to wait 4 hours after dosing before breastfeeding.32 It should be noted that medium to large doses of systemic corticosteroids have been reported to temporarily decrease lactation.33
Studies suggest that corticosteroid monotherapy in early-stage Vogt-Koyanagi-Harada disease often fails to prevent recurrence and serious complications like subclinical choroiditis and progression to “sunset glow fundus,” supporting the use of additional immunosuppressive therapy for improved long-term outcomes.34,35 Synthetic disease-modifying antirheumatic drugs considered safe for use during pregnancy and lactation include hydroxychloroquine, chloroquine, azathioprine, colchicine, intravenous immunoglobulin, and tacrolimus.36 Infants born to mothers who received hydroxychloroquine during pregnancy and breastfeeding showed no significant congenital malformations, and all infants, including those who were breastfed, demonstrated normal visual function and neurodevelopmental outcomes.37 Cyclosporin A can be used at doses ranging from 2.5 to 5 mg per kg per day for severe uveitis in pregnant women requiring immunosuppressive therapy and is compatible with breastfeeding.38,39 In contrast, the use of methotrexate, cyclophosphamide, and nonspecific immunomodulators, such as mycophenolate mofetil and leflunomide, is not recommended during pregnancy and lactation because of their teratogenic profile and lack of data in breasted infants.30,40 Biologic disease-modifying antirheumatic drugs such as tumor necrosis factor inhibitors, including infliximab, etanercept, and certolizumab pegol, are generally considered safe in pregnancy with little, if any, drug passing to the infant during lactation.40,41
Managing Vogt-Koyanagi-Harada disease, particularly in pregnant and postpartum patients, requires a multidisciplinary approach because of the complexity of the condition and the potential for systemic involvement. In addition to optometric care for the ocular manifestations of Vogt-Koyanagi-Harada disease, coordination with internal medicine, retinal specialists, rheumatology, and obstetrics is critical. The collaborative effort between these specialties ensures comprehensive care that addresses both the ocular and systemic aspects of Vogt-Koyanagi-Harada disease while also managing the unique considerations of pregnancy and the postpartum period, where hormonal changes can influence disease activity. Furthermore, the course of treatment may be critical in reducing recurrence rates. A retrospective study involving 35 patients with Vogt-Koyanagi-Harada disease treated with oral corticosteroids revealed that those who received treatment for less than 6 months had a significantly higher recurrence rate (58.8%) compared with those treated for 6 months or longer (11.1%).42
Although breastfeeding has been shown to have a multitude of beneficial effects for the baby and mother, this patient was advised to stop breastfeeding for 2 reasons. We anticipated an extended course of high-dose systemic prednisone, and the potential risks associated with prolonged exposure to high levels of corticosteroids could pose a threat to the infant’s health and the mother’s milk supply.33 Secondly, discontinuing breastfeeding can help rebalance the immune system, potentially benefiting conditions driven by type 1 T helper cell–mediated pathways, such as certain autoimmune diseases. This shift may reduce inflammation in type 1 T helper cell–mediated conditions, suggesting a therapeutic benefit from weaning in these contexts.43 Additionally, the relationship between prolactin and increased inflammatory activity during the postpartum period suggests that by returning hormone levels to baseline, the immune system may stabilize, possibly reducing the activity of some autoimmune diseases.
Our case exemplifies the significant challenges both patients and practitioners face when access to comprehensive health care is limited, particularly for uninsured individuals. In this instance, additional imaging modalities such as magnetic resonance imaging, computed tomography, and chest x-ray would have provided valuable diagnostic insight. However, due to the patient’s lack of insurance, these tests were cost prohibitive, forcing the health care team to rely primarily on clinical findings, ophthalmic imaging, and the patient’s response to treatment. The inability to use more advanced diagnostic tools underscores the barriers to care that uninsured patients encounter, often leading to delayed or incomplete diagnoses. This highlights the need for more affordable and accessible diagnostic options, particularly in complex autoimmune conditions like Vogt-Koyanagi-Harada disease, where early and accurate diagnosis is crucial to prevent long-term complications.
CONCLUSION
The postpartum period is a vulnerable time for women, during which they are at increased risk of developing autoimmune diseases and associated ocular disorders. Managing noninfectious uveitis during pregnancy and the postpartum period is complex, requiring careful consideration to balance the health of the mother and baby. This case demonstrates the clinical course of a postpartum female with Vogt-Koyanagi-Harada disease that responded well to oral prednisone. This case also illustrates the increased susceptibility of recurrence with short-term use of systemic corticosteroids. The patient experienced a worsening of the clinical signs and symptoms after she abruptly discontinued oral prednisone 78 days after starting treatment. Practitioners should educate their patients on the anticipated course of treatment to help promote compliance. Considering the variations in autoimmune conditions during pregnancy and the postpartum period, further research is needed to optimize diagnostic and treatment strategies for these patients.
TAKE HOME POINTS
-
Hormonal and immune system fluctuations during and after pregnancy can increase the risk for autoimmune disease and noninfectious uveitis in postpartum women.
-
Breastfeeding can further exacerbate autoimmune disease due to increased prolactin levels that can lead to changes in immune response.
-
Managing Vogt-Koyanagi-Harada disease in pregnant or lactating women requires balancing maternal and baby’s health, with nonfluorinated glucocorticoids and specific disease-modifying antirheumatic drugs being safer options.
ACKNOWLEDGMENTS
The authors thank Mark Bronstein, MD, for his contribution to the clinical care of this patient.