


INTRODUCTION
Bartonella henselae neuroretinitis represents a common infectious etiology of painless vision loss. Although self-limiting, prompt treatment is imperative in shortening the course of active infection and preventing permanent vision loss.1 B henselae is a subspecies within the Bartonella genus. This organism can reside asymptomatically in the saliva of host cats or kittens and is transmitted to humans through direct contact via bites or scratches or indirectly via arthropod vectors such as infected fleas or ticks. B henselae, along with other species in the Bartonella genus, is a Gram-negative, hemotropic bacteria requiring migration to host cells for replication.2,3
The infection most commonly produced by transmission of B henselae is referred to as cat scratch disease and unfolds in several distinct stages. Initially, B henselae gains entry into the host through a mechanical vector, typically a scratch or bite from an infected cat, and subsequently disseminates to regional lymph nodes. To establish infection, B henselae must circumvent the host’s immune defenses and modulate apoptotic pathways to prevent apoptosis in the infected cells, which predominantly include macrophages, erythrocytes, and vascular endothelial cells.3 Within these cells, B henselae proliferates inside membrane-bound vacuoles. The bacterium’s capacity to invade and persist in erythrocytes and vascular endothelial cells is related to its pathogenicity, contributing significantly to the disease’s clinical manifestations.3
The typical presentation of cat scratch disease includes erythematous papules at the entry site and enlarged lymph nodes. Fever, lethargy, and visceral organ involvement may occur due to the invasion of endothelial cells and erythrocytes.4 Aside from systemic lymphadenopathy, cat scratch disease may result in ocular manifestations since the eye is the second most affected site after the lymphatic system.5 B henselae may enter the eye through facial scratches or inoculation of the conjunctiva. This accounts for 5% to 7% of cat scratch disease cases.6 Although any layer of the eye can be affected by cat scratch disease, the 2 most common ocular manifestations in immunocompetent patients are Parinaud’s oculoglandular syndrome and neuroretinitis.
Parinaud’s oculoglandular syndrome refers to unilateral follicular conjunctivitis and ipsilateral lymphadenopathy. Other signs of Parinaud’s oculoglandular syndrome include periorbital edema, mucus discharge, conjunctival ulceration overlying a granuloma, and rarely corneal ulceration. Lymphadenopathies may be preauricular or postauricular, cervical, or submandibular. As with typical cat scratch disease infections, low-grade fevers, or malaise may be present. Parinaud’s oculoglandular syndrome is self-limiting after several weeks.6
A posterior segment study of 35 eyes with cat scratch disease neuroretinitis by Solley et al described white retinal lesions as the most prevalent ocular finding, seen in 83% of eyes. This was followed by optic disc edema in 46% of eyes, a macular star in 43% of eyes, and vascular occlusive events in 14% of eyes associated with the areas of white retinal lesions.7,8 These observations are not pathognomonic for cat scratch disease and necessitate further investigative measures to rule out other visually significant and potentially threatening conditions. No identifiable health information was included in this case report.
CASE REPORT
A 46-year-old White man presented to the eye clinic, referred from the emergency department, complaining of a gradual reduction in vision in the right eye more than the left eye over the past week, a central scotoma in the right eye, pressure in both eyes, and generalized headaches. His ocular history was notable only for hyperopia, astigmatism, and presbyopia. He denied previous ocular surgeries or trauma, and he was not using any ophthalmic medications. His medical history included asthma, non–insulin-dependent diabetes mellitus, and gastroesophageal reflux disease, for which he was taking metformin and omeprazole. The patient denied the use of tobacco and alcohol but disclosed occasional marijuana use. His point-of-care glucose test measured in the emergency department was high at 143 mg/dL and his blood pressure was 131/72 mm Hg, which was down from the previous reading of 163/90 mm Hg. The patient was considered morbidly obese for his stature although he had no significant weight gain in the past couple of years.
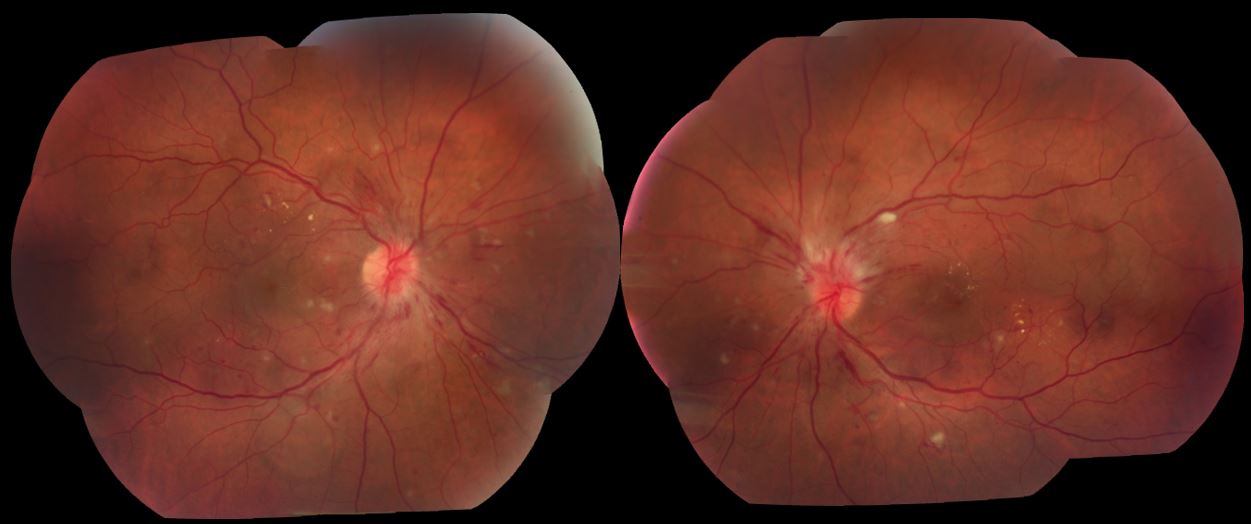
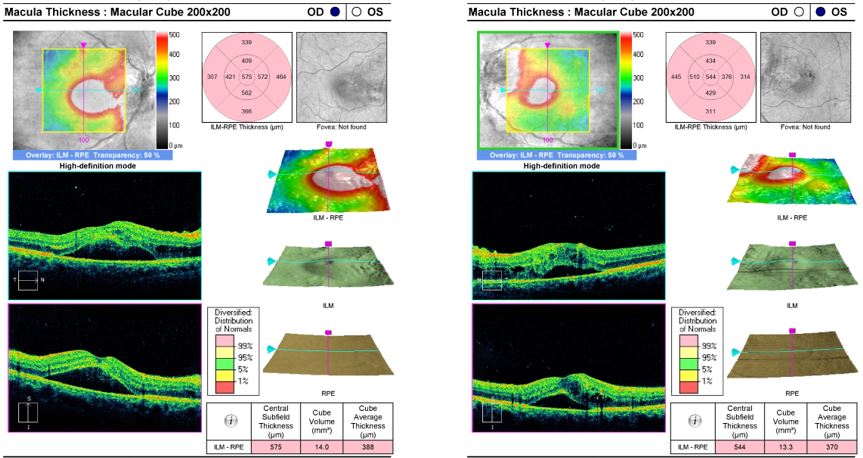
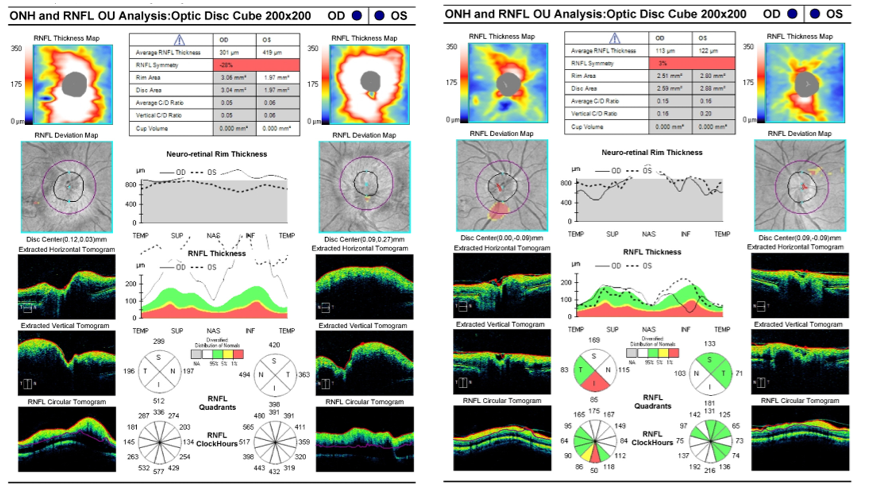
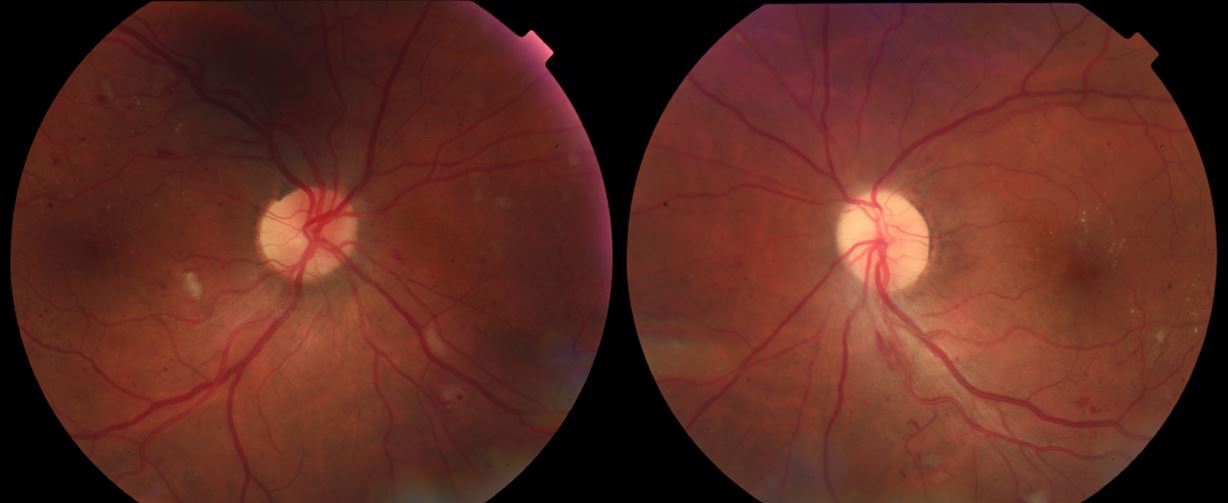
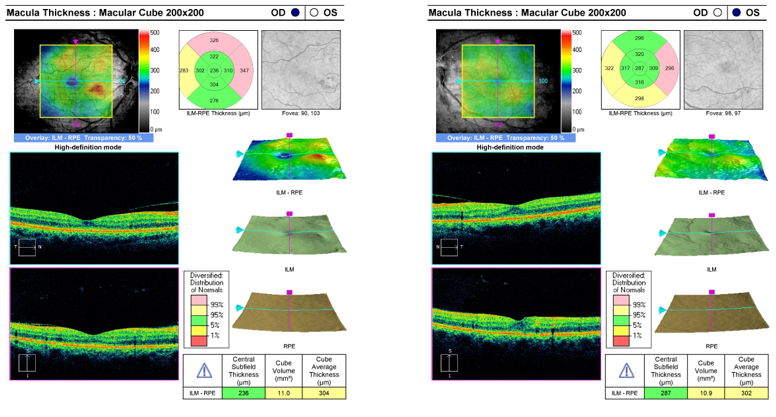
On examination, his best-corrected Snellen visual acuity was 20/400 in the right eye and 20/20 in the left eye, with a correction of +1.00+0.50×120 in the right eye and +1.00+0.50×060 in the left eye. His pupils were reported by the ophthalmic technician to be round, equally reactive, and without a relative afferent pupillary defect; however, the patient was dilated before an evaluation by the doctor. He was full on confrontation visual field testing in each eye and had full extraocular motilities in both eyes. Intraocular pressures were measured by Tono-Pen at 18 mm Hg in the right eye and 19 mm Hg in the left eye. Slit lamp examination of the anterior segment was unremarkable in both eyes. Fundus examination of both eyes alike was remarkable for hyperemic optic nerve edema, venous dilation, arteriovenous nicking, scattered intraretinal hemorrhages, multiple cotton wool spots, and macular edema (Figure 1). Optical coherence tomography of the macula in both eyes demonstrated subfoveal subretinal fluid and pockets of intraretinal fluid (Figure 2). Assessment of the retinal nerve fiber layer on optical coherence tomography showed robust thickening across all quadrants, with an average thickness of 301 µm in the right eye and 419 µm in the left eye, which is indicative of bilateral optic nerve edema (Figure 3).



At this juncture, differential diagnoses considered included diabetic papillitis and retinopathy, hypertensive retinopathy, ischemic optic neuropathy, neuroretinitis, tuberculosis, syphilis, sarcoidosis, leukemia, lymphoma, and elevated intracranial pressure. Upon probing, the patient denied having any known exposure to tuberculosis and denied recent sexual activity with new partners. He did endorse, however, owning a cat and having been recently scratched several times. Because of the broad list of differentials, this patient’s case was co-managed between optometry, ophthalmology, and neuro-ophthalmology. Urgent imaging of the brain and orbits were ordered as well as a slew of infectious and inflammatory laboratory testing, including Bartonella titers, and the patient was directed to return to the eye clinic in 1 week for review.
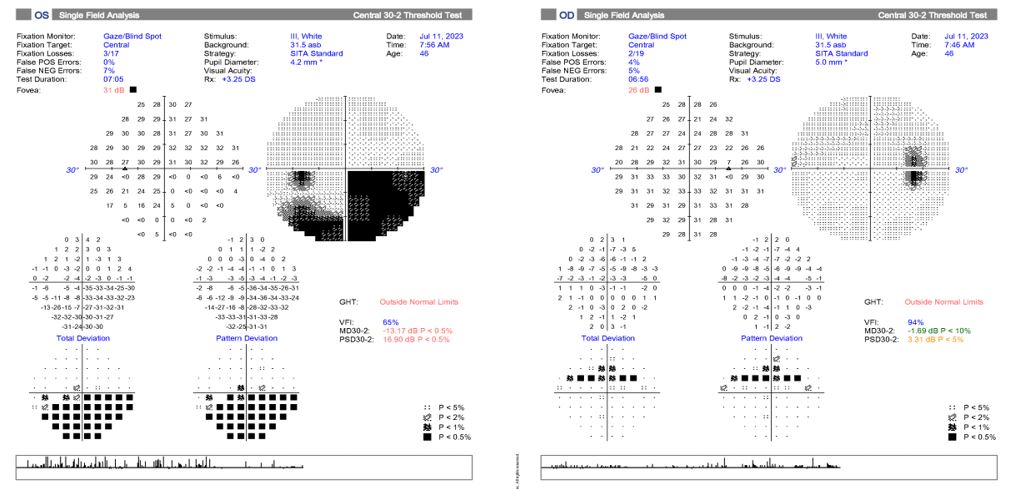
At the 1-week follow-up appointment, the patient reported improved vision in both eyes and a smaller central scotoma in the right eye. His best-corrected Snellen visual acuities were measured at 20/40 in the right eye and 20/25+2 in the left eye with a stable prescription. Intraocular pressures remained normal at 14 mm Hg in both eyes via Tono-Pen. Humphrey visual field 30-2 yielded a reliable inferior altitudinal defect in the left eye and superior field misses in the right eye (Figure 4). This was consistent with the afferent pupillary defect in the left eye eventually noted at this follow-up examination. A subsequent optical coherence tomography of the retinal nerve fiber layer was remarkable for persistent thickening in all quadrants, although average thicknesses decreased to 294 µm in the right eye and 343 µm in the left eye. Repeat dilation of both eyes revealed persistent findings of nonproliferative diabetic retinopathy, hypertensive vascular changes, macular edema, and disc edema.


Review of the magnetic resonance imaging of the brain and orbits with and without contrast and magnetic resonance venography showed no retrobulbar pathology or intracranial processes. The patient’s A1c had returned at 7.4%, down from 9.3% 3 years prior. Serology results revealed a nonreactive rapid plasma reagin, no treponemal detection on fluorescent treponemal antibody absorption, an angiotensin-converting enzyme within range and lysozyme levels within normal limits. At this time, the QuantiFERON tuberculosis test and Bartonella serology were collected but results had not yet been completed.
The patient was started on provisional oral doxycycline 100 mg twice daily given recent cat scratches while pending the Bartonella serology. He was also started on a short-term course of oral acetazolamide 1000 mg once daily given bilateral disc edema, headaches, and obesity. A lumbar puncture was ordered, and the patient was again scheduled to return to the eye clinic in 1 week.
Prior to his follow-up appointment, the QuantiFERON tuberculosis test came back negative and Bartonella serology came back positive. The immunoglobulin G henselae titer was significantly elevated at 1:1024 compared with the normal range of 1:64 or less, confirming current infection. The immunoglobulin M titer was 1:20, which is considered out of range as well. The final serology results are organized in Table 1. The patient missed his 1-week follow-up appointment and rescheduled for a later date.
Two weeks later, the patient returned to the eye clinic and reported compliance with doxycycline 100 mg twice daily and acetazolamide 1000 mg once daily since his last visit 3 weeks prior. He reported improvement in the pressure sensation of both eyes and improved vision. He had no new visual or ocular symptoms. His entrance tests, visual acuity, and intraocular pressure remained stable at this visit. A dilated fundus examination revealed persistent but improved optic nerve edema and nonproliferative retinopathy with persistent macular edema in both eyes. He ultimately declined the lumbar puncture; however, neuro-ophthalmologic examination and magnetic resonance imaging findings were not suspicious for intracranial hypertension. He was instructed to discontinue acetazolamide and continue doxycycline 100 mg twice daily for an additional 30 days.
He returned to the eye clinic as scheduled, and after 1 additional month on doxycycline alone, his best-corrected Snellen visual acuities significantly improved in the right eye and remained excellent in the left eye: 20/20 in each eye with a final refraction of +1.00+0.50×135 in the right eye and +0.50+0.50×040 in the left eye. Entrance testing remained the same. Intraocular pressure remained within normal limits in each eye. The anterior segment examination was similarly unremarkable in both eyes. An undilated examination with a 90-D lens revealed trace temporal optic nerve pallor in the right eye and significant optic nerve pallor in the left eye with no signs of edema in either eye (Figure 5). Repeat optical coherence tomography of the optic nerves demonstrated a much less thickened retinal nerve fiber layer compared with baseline (Figure 3). Humphrey visual field 30-2 showed a persistent inferior altitudinal defect in the left eye and superior field misses in the right eye. Optical coherence tomography of each macula indicated normal foveal contour and resolved central edema despite persistent retinopathy (Figure 6).


Given positive Bartonella serology with high titers, an established cat scratch history, and confounding vascular comorbidities, the patient was diagnosed with bilateral neuroretinitis due to B henselae with superimposed diabetic and hypertensive retinopathy. He was advised to follow up in the eye clinic in 3 months and to follow up routinely with his primary care doctor for continued care of his vascular comorbidities. He was also referred to the infectious disease department for continued management of Bartonella infection. Unfortunately, the patient cancelled his follow-up appointment in the eye clinic and did not schedule an infectious disease appointment.
DISCUSSION
Neuroretinitis of all types typically presents unilaterally; however, it can present bilaterally as shown in this case. It generally affects younger individuals aged between 8 and 40 years and tends to affect females more than males.9 Optic nerve edema is a classic finding in neuroretinitis, although it can also be observed in several other conditions. Common noninfectious differentials of optic nerve edema include hypertension, diabetes mellitus, retinal vein occlusion, elevated intracranial pressure, and anterior ischemic optic neuropathy. Infectious differentials include syphilis, toxoplasmosis, Toxocara, Lyme disease, herpes virus, and Bartonella species.10 White retinal lesions and macular star formation are additional common findings in neuroretinitis, although they were not appreciated in our patient. The absence of a macular star was also noted in a case report by Saxena et al in a patient with visual changes and significantly elevated B henselae serology, further demonstrating the possible variability in neuroretinitis presentation as we know it. In addition to bilaterality, lack of macular star formation, lack of retinal white lesions, and confounding vascular etiologies, our patient did not have any systemic symptoms common in cat scratch disease such as fever, lethargy, or erythematous skin papules, making for an unusual case of B henselae neuroretinitis. Nevertheless, a thorough patient history, including possible instances of infectious transmission and medical history, as well as imaging and comprehensive serology testing, facilitated proper differentiation and diagnosis.
Bartonella species are notoriously challenging to culture in vitro. The optimal method for noninvasive detection of these bacteria is through serological testing, utilizing techniques such as the indirect fluorescent antibody (IFA) assay or the enzyme-linked immunosorbent assay. These methodologies are essential for confirming the presence of Bartonella in clinical specimens. Serological testing involves the detection of specific antibodies, namely immunoglobulin G and immunoglobulin M, in the bloodstream that target distinct antigens of Bartonella spp. Serological assays that yield a titer below a predetermined threshold for a specific antigen indicate a negative test result. This method facilitates the identification of immune responses to Bartonella infections, providing important diagnostic information. A positive indirect fluorescent antibody for immunoglobulin M, in the case of Bartonella, will show a predictive value greater than 1:20.11 This would indicate a positive result and active infection of either B henselae or B quintana. Serology testing for immunoglobulin G titers will indicate a current or previous infection of Bartonella.
Treatment of B henselae infection is contingent upon several critical factors. Although focal and systemic infections generally exhibit a self-limiting course, therapeutic intervention is recommended to mitigate potential complications and facilitate recovery.12,13 In immunocompetent individuals, active infection with B henselae typically resolves within 4 to 6 weeks. In immunocompromised patients, however, resolution of the infection may extend up to 4 months.14 Age must also be considered when prescribing antibiotics. Macrolides are preferred in children 8 years old and under because of the side effects of doxycycline. In adults, doxycycline and rifampin showed the potential to quicken resolution.15 Therapeutic regimens for this condition may include the administration of antibiotics such as azithromycin, trimethoprim-sulfamethoxazole, gentamycin, and ciprofloxacin. A concurrent oral corticosteroid may be prescribed as well. Clinical studies have demonstrated that combining an antibiotic with an oral steroid improves visual recovery in 88% of affected eyes compared with 50% using antibiotics alone.16 A steroid was not initiated for our patient given significant improvement in vision and symptoms with antibiotics alone.
The Centers for Disease Control and Prevention website delineates primary prevention strategies for Bartonella infection. These recommendations include avoiding scratches, bites, and licks from felines, particularly kittens and stray cats. Additionally, it is advised that immunocompromised individuals refrain from acquiring cats aged younger than 1 year.17
CONCLUSION
B henselae is recognized as an infectious etiology of neuroretinitis, which can lead to painless vision loss. The disease course tends to be self-limiting, although prompt treatment may shorten infection time and prevent permanent visual symptoms. Ocular manifestations include white retinal lesions, optic disc edema, macular star, and vascular occlusive events. Several infectious and noninfectious etiologies may present the same way and must not be overlooked. Moreover, the possibility of compounded diagnoses should not be excluded as patients may present with concurrent systemic conditions. A thorough patient history, including possible infectious transmission and medical history, as well as imaging and comprehensive serology testing, can facilitate proper diagnosis and management of neuroretinitis caused by B henselae. Doxycycline and rifampin are standard antibiotic treatment options for adults, whereas macrolides prove safer for adolescents. Preventative measures to evade infection with B henselae include avoiding scratches, bites, and licks from felines.
TAKE HOME POINTS
-
Neuroretinitis caused by Bartonella henselae commonly presents with optic nerve edema and, although typically unilateral, can manifest bilaterally.
-
In addition to serology, a comprehensive medical history, including possible infectious transmission, is key to properly diagnosing neuroretinitis caused by B henselae.
-
B henselae neuroretinitis is naturally self-limiting, yet prompt treatment may shorten infection time and prevent lasting visual symptoms.
-
Neuroretinitis can commonly mimic vascular retinal disease. The possibility of compounded diagnoses should not be excluded as patients may present with concurrent systemic conditions.