



Introduction
Losartan is a US Food and Drug Administration–approved treatment for hypertension, diabetic neuropathy, and hypertension with left ventricular hypertophy.1,2 When administered systemically, losartan acts as an angiotensin receptor blocker, which has several effects on the body, some of which include angiotensin II–induced vasopressin release, inhibition of angiotensin II–induced vasoconstriction, and promotion of renoprotective effects in patients with type II diabetes.1 Although losartan has been in the market for decades, it has recently been consider by eyecare professionals for treating corneal haze after traumatic injury, microbial infections, postsurgical complications, and persistent corneal epithelial defects.3,4
Losartan’s ophthalmic use stems from this drug’s ability to act on corneal myofibroblasts, which are known to produce large amounts of disordered corneal extracellular matrix; this subsequently produces corneal stromal scaring/fibrosis/haze while also potentially inhibiting corneal epithelial healing.4 Losartan is thought to act on the cornea by inhibiting transforming growth factor beta activity, which is a cytokine linked to the fibrotic processes.3 Transforming growth factor beta stimulates collagen synthesis (types I and III), and treatment with losartan reduces corneal collagen deposition.3 With corneal healing, topical losartan is thought to act by inhibiting transforming growth factor beta-1 and transforming growth factor beta-2 signal transduction molecule erk.5 Topical losartan then likely causes myofibroblasts to undergo apoptosis, which subsequently decreases corneal haze.6 After myofibroblast removal, corneal fibroblasts migrate into the affected tissue to reabsorb and reorganize the disordered corneal extracellular matrix.2 Keratocytes then move into the damage tissue to reorganize the corneal stroma to promote normal corneal function.2 Losartan may likewise inhibit inflammation, which could further promote corneal transparency.3 Corneal epithelial cells furthermore release mediators that promote neovascularization, which recruits myofibroblasts; thus, topical losartan may have benefits for treating neovascularization.3
This mechanistic theory is supported by a series of rabbit studies and case reports. Sampaio et al (2022) were the first to use the rabbit model to evaluate the usefulness of topical losartan for the treatment of late corneal haze by evaluating rabbits that were treated with high-correction photorefractive keratectomy (-9.00 D induced), postcorneal challenge with a severe alkali burn, or surgically induced, highly irregular corneal injuries (mimicking combat injury) in 3 independent studies.7–9 The authors evaluated each of these situations by treating the eyes with topical losartan in saline 6 times per day for 1 month or just with saline.7–9 With all studies, the authors found that myofibroblasts were reduced, yet they only found corneal haze to be reduced during the photorefractive keratectomy and alkali burn challenges.7,8 The likely reasons for no reduction in corneal haze with highly irregular corneal injuries was simply that the corneal shape was just too irregular, which suggests that highly irregular corneas should be surgically smoothed before treatment.9 A pair of rabbit studies from Martinez et al support the above work. Martinez et al specifically furthered the field by challenging rabbits’ eyes with an alkali burn and allowed the eyes to heal for 1 month to mimic human late-phase corneal fibrosis/haze.6 Eyes were treated with topical losartan and compared to eyes treated with saline, with the authors finding that topical losartan was able to significantly lessen haze and myofibroblasts 1 month after treatment.6 Martinez et al repeated this experimental set up by challenging corneas with “radial, nearly full-thickness incisions from the center of the cornea and into the limbus” to evaluate how topical losartan would affect wound closure. Corneas were immediately treated this time, with the authors determining that topical losartan did not inhibit corneal lesion closure with it also significantly decreasing myofibroblasts.5
These basic science experiments set the stage for clinically using topical losartan. When administered as an off-label treatment for corneal haze, topical losartan is compounded by dissolving it in a balanced salt solution at a concentration of 0.8 mg/mL and dosed 6 times daily.4 This approach has been previously used by Pereira-Souza et al to treat a 36-year-old female who had developed “late haze” after LASIK surgery.10 The treated patient had a dense layer of subepithelial haze in her affected eye while presenting with a visual acuity of 20/200.10 The patient was subsequently treated with 0.8 mg/mL topical losartan for 4.5 months with the patient having a significant reduction in corneal haze and an improvement in corrected visual acuity to 20/25. Rodgers et al later encountered a 20-year-old male patient who had clinically significant corneal haze after corneal crosslinking for keratoconus.11 The patient had persistent haze 107 days after treatment in his right eye, which resulted in an uncorrected visual acuity of 20/150.11 The patient was then treated 6 times per day with 0.8 mg/mL topical losartan for 3 months, with the authors finding a significant reduction in corneal haze and an improvement in visual acuity to 20/40.11 Although there is both basic science and clinical cases supporting the use of topical losartan for treating corneal haze, anecdotally not all patients respond to this innovative treatment. Thus, the authors will present a case in which a patient was successfully treated with topical losartan and a case in which a patient was unsuccessfully treated with topical losartan with the article closing with a discussion of when to best use topical losartan for treating corneal haze.
POINT: Clinical Case Supporting Topical Losartan for Treating Corneal Haze
Case History
-
White man, aged 72 years
-
Patient complained of blurred vision in left eye
-
Patient had history of stromal herpes keratitis infection 4 years prior
Examination Findings
-
Visual Acuity Without Correction:
-
Right eye: 20/400
-
Left eye: 20/20
-
-
Manifest Refraction:
-
Right eye: +2.00 -6.00 × 152, 20/400
-
Left eye: 0.00 sphere, 20/20
-
-
Slit Lamp Examination:
-
Lids/lashes: clear in each eye
-
Conjunctiva: 3+ hyperemia in right eye, clear in left eye
-
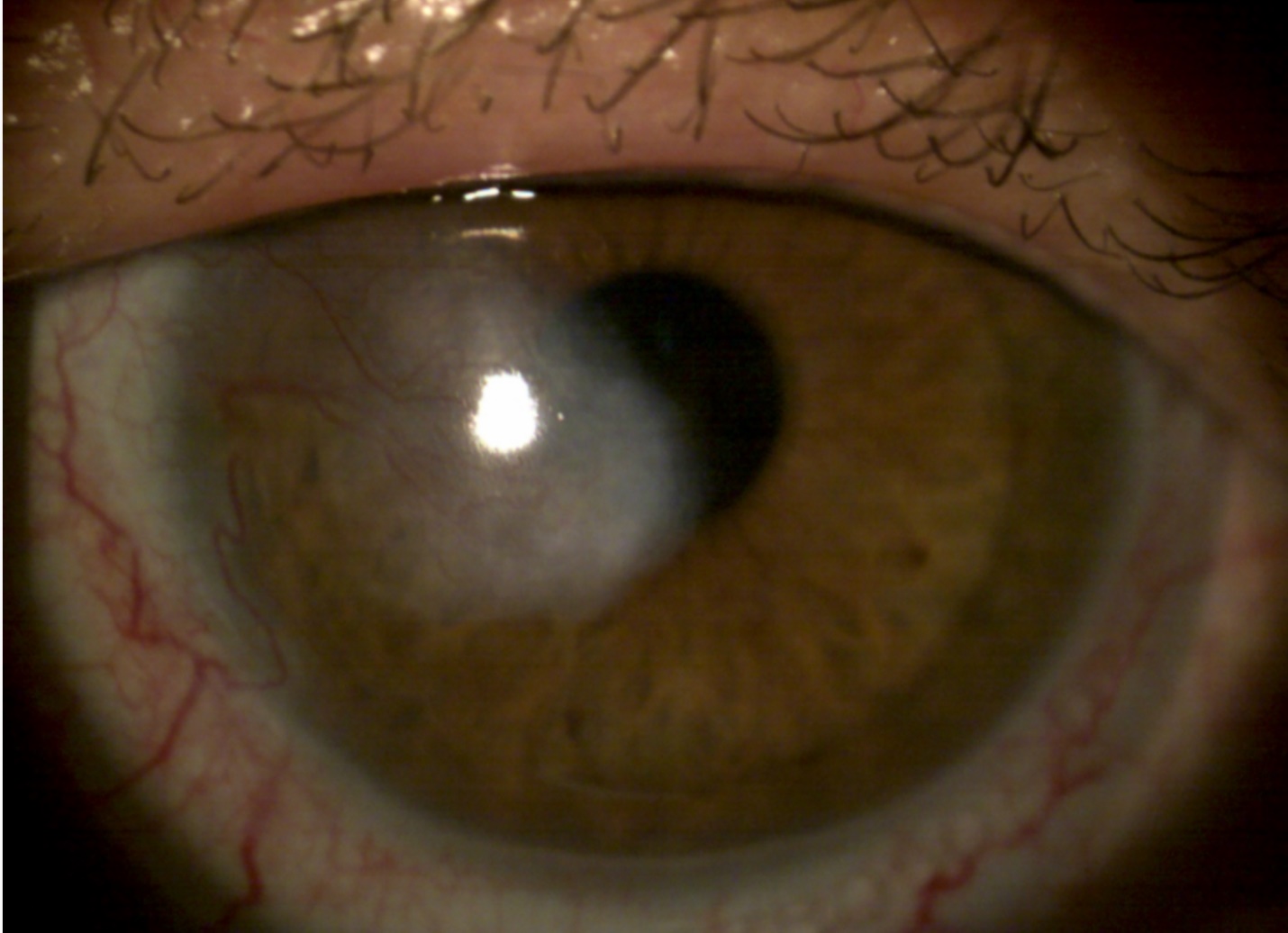
Cornea: dense stromal scar with ectasia and neovascularization in right eye (Figure 1), clear in left eye
-
Anterior Chamber: deep and quiet in each eye
-
Iris: flat brown in each eye
-
Lens: 2 + nuclear sclerosis in each eye
-

A 72-year-old White man with a history of unilateral corneal scarring from herpes zoster stromal keratitis was referred to a private practice optometry clinic for continued care. During care, the patient’s affected right eye was prescribed a scleral lens. The lens device provided the scarred corneal surface with visual rehabilitation and protection for 2 years before the forthcoming topical losartan treatment. With scleral lens wear, vision improved to 20/40. This patient also suffered from symptoms of dry eye disease for which he was prescribed cyclosporine ophthalmic emulsion 0.05% and artificial tears in the form of carboxymethylcellulose 0.5% ophthalmic solution. Both topical medications were placed directly on the eye, before and after lens wear, twice a day, in both eyes.
In attempts to improve vision, the patient elected treatment with topical losartan 0.08% ophthalmic solution. As already mentioned, topical ophthalmic losartan was reported to improve corneal scarring in noncontact lens wearing patients at the dosing of 6 times per day.4 Nevertheless, because the patient’s uncorrected visual acuity was poor, he requested uninterrupted daytime wearing of scleral lenses during topical losartan treatment. To accommodate the patient’s habitual lens wear schedule, topical losartan treatment was therefore prescribed twice a day. The first dose was applied to the bowl of the scleral lens before device insertion, whereas the second dose was placed directly onto the eye after nighttime lens removal. Dosing into the scleral lens bowl was as followed: 1 drop of topical losartan ophthalmic solution 0.08% followed by 4 drops of balanced saline solution in the form of 0.09% sodium chloride inhalation solution.
The aqueous vault of a scleral lens can be combined with topical ophthalmic medication for aiding the treatment of ocular surface disease. For example, scleral lenses have been filled with topical ophthalmic antibiotics and corticosteroids, autologous serum, and antivascular endothelial growth factors.12–14 Using a scleral lens as a drug delivery device allows for an increase in the bioavailability of medication to the ocular surface.15 Therefore, using the patient’s own scleral lens to deliver topical losartan treatment to reduce corneal scarring seemed likely to succeed.
Figure 1 shows the patient 2 months before topical losartan treatment. After 2 months of use, the patient’s uncorrected acuity improved to 20/150 and scleral lens corrected acuity improved to 20/25. In addition, there was markedly less conjunctival hyperemia and corneal neovascularization (Figure 2). After 5 months of topical losartan dosing, the scleral lens vision improved to 20/20 but his uncorrected vision remained unchanged. Also, at this visit, the patient subjectively reported that his cornea appeared more transparent and conjunctiva less hyperemic (Figure 3). Because the patient’s acuity and ocular appearance were still improving, topical losartan treatment was continued until his next follow-up visit scheduled for 2 months.


This case illustrates the successful use of topical ophthalmic losartan for improving corneal scarring from herpes zoster stromal keratitis in a scleral lens wearing patient. The author, who is also the patient’s provider, would like to share several notable observations made during topical losartan 0.08% ophthalmic solution treatment:
-
Objective and subjective decreased corneal scarring
-
Improved uncorrected and corrected visual acuity
-
Objective and subjective improved conjunctival hyperemia
-
Decreased corneal neovascularization
-
Good safety and subjective patient ease using scleral device for drug delivery
COUNTERPOINT: Clinical Case Against Topical Losartan for Treating Corneal Haze
Case History
-
White woman, aged 43 years
-
Patient complained of blurred, hazy vision in the right eye more than in the left eye that fluctuates throughout the day
-
Patient had a history of photorefractive keratectomy in each eye (2012) with enhancement in each eye (February 2023)
-
Scleral buckle in right eye (2007)
-
Used Xdemvy in the past for blepharitis
Examination Findings
-
Visual Acuity Without Correction
-
Right eye: 20/25-1, J3
-
Left eye: 20/20-1, J2
-
-
Manifest Refraction:
-
Right eye: +1.00 -0.75 × 145, 20/20-2 “fuzzy”
-
Left eye: -0.25 sphere 20/20
-
-
Slit Lamp Examination:
-
Lids/lashes: no collarettes, clear in each eye
-
Conjunctiva: white and quiet in each eye
-
Cornea: no staining, 1+ central reticular haze in right eye and trace reticular haze in left eye
-
Anterior chamber: deep and quiet in each eye
-
Iris: flat brown in each eye
-
Lens: clear in each eye
-
The patient was diagnosed with corneal opacity that was worse in the right eye than the left eye corresponding to late-onset corneal haze following photorefractive keratectomy. Treatment options were discussed with the patient including topical steroids, 0.8 mg/mL topical losartan, or superficial keratectomy with mitomycin C. It had been more than 10 months since the patient’s photorefractive keratectomy enhancement. The patient elected for conservative treatment and was prescribed losartan 0.8 mg/mL 6 times per day in each eye for 1 month then 3 times per day for another month until her follow-up visit.
The patient returned 10 weeks later. She was taking the losartan drops 3 times per day in each eye. Her uncorrected vision was stable from her previous examination. She was unsure whether she noticed any improvement since using the topical losartan. The corneal appearance on slit lamp examination appeared unchanged from 10 weeks prior (Figure 4). The patient indicated she did not feel the losartan was beneficial and did not want to continue with the treatment.


Corneal haze following photorefractive keratectomy results from an inflammatory response as the eye heals from the surgically induced trauma.3 As part of stromal healing, molecules within the resulting extracellular matrix cause disorganization within the tissue inhibiting corneal clarity. Further haze formation can result from prolonged myofibroblast proliferation and excessive extracellular matrix formation. In this case, topical losartan was not effective in treating the late-stage post–photorefractive keratectomy haze. The treatment was discontinued at the patient’s request because of the lack of perceived benefit from both the patient and examiner perspective. Although this case demonstrated limited efficacy during the first 10 weeks of treatment, this limited efficacy could partly be due to the relatively short duration of treatment compared with other cases described in the literature and the successful case described above.10,11
Conclusion
Corneal haze or opacification may develop following trauma, infection, inflammation, or corneal surgery.16 There are several management options for corneal opacification, including topical corticosteroids, surgical procedures, and now topical losartan.10,16 Some practitioners and patients may feel more comfortable beginning with conservative approaches prior to proceeding with corneal surgery to treat corneal haze, particularly early-stage haze.
Topical corticosteroids and mitomycin C have been used to treat corneal haze status after refractive surgery and to prevent recurrence of haze.10,16,17 Topical corticosteroids improve corneal haze by reducing inflammation, and mitomycin C reduces the proliferation of myofibroblasts.16,17 However, mitomycin C is more commonly used prophylactically after refractive surgery and is not as effective in treating long-standing corneal opacifications.10 Although topical corticosteroids are commonly prescribed to treat postoperative inflammation, long-term use is discouraged because of potential side effects.10 Therefore, the off-label use of compounded 0.8 mg/mL topical losartan dosed 6 times per day may be considered a more conservative approach in treating patients with corneal haze and appealing to some practitioners as its mechanism of action is thought to be similar to previous conservative approaches and have fewer known long-term side effects.5,7,9,10 The 2 cases presented in this point-counterpoint highlight the visual challenges that some patients experience secondary to corneal haze.
The first patient exhibited both subjective improvement in clarity of vision and objective reduction of corneal opacification with use of ophthalmic losartan in conjunction with scleral lenses. The use of losartan in this case supports the currently accepted mechanism of topical losartan causing corneal myofibroblasts to undergo apoptosis, thereby decreasing corneal haze.5,7,9,10 This case supports other published reports that topical losartan may be therapeutic in reducing corneal haze and may be an alternative therapy than previously accepted.10
The second patient developed late-onset corneal opacification after photorefractive keratectomy (more than 10 months after photorefractive keratectomy enhancement). Although the patient used compounded 0.8 mg/mL topical losartan for 2 months, the treatment was ultimately discontinued. Both the patient and clinician failed to see improvement in corneal haze with topical losartan use. Studies have shown that only 5% to 15% of patients with late-haze corneal opacification status after refractive surgery demonstrate a decrease in haze when treated with topical corticosteroids.10,18 Topical losartan may also not be effective for late-haze corneal opacification, especially when the patient has a highly irregular cornea, based on the mechanism of action, past animal studies, and lack of clinical improvement found in this clinical case.9
Ultimately, the efficacy of topical losartan may depend on the underlying cause of corneal haze, presence or absence of neovascularization, and duration the haze has been present. For long-standing corneal opacifications, topical losartan may not be considered an initial treatment because of the cost and time involved in having the medication made by a compounding pharmacy as well as the lack of improvement in reduction of corneal haze. In these cases, other management options may be preferred. Additional case reports and clinical trials are needed to determine the benefit of topical losartan in the management of corneal haze.
Take home POints
-
Although topical losartan is not a first-line treatment, there is evidence indicating that it is effective in both animals and humans for treating recalcitrant corneal haze.
-
Topical losartan can be effectively delivered with scleral lenses.
-
Topical losartan may not be effective in patients who have highly irregular corneas.
-
Randomized clinical trials are still needed to fully vet topical losartan as a treatment for recalcitrant corneal haze.
Patient consent
No identifiable health information was included in this point counter point.
Conflicts of Interest
The authors have received research support from AbbVie Pharmaceuticals (A.D.P.), Alcon Research, LLC (A.D.P., J.S.H.), Art Optical (J.S.H.), Bausch + Lomb (A.D.P., J.S.H.), Contamac (J.S.H.), Euclid (J.S.H.), International Keratoconus Academy (J.S.H.), and Ocular Therapeutix (J.S.H.). The authors have served as consultants for AbbVie Pharmaceuticals (J.S.H.), Alcon (A.D.P., J.S.H.), Bausch + Lomb (A.D.P.), CooperVision (J.S.H.), Euclid (J.S.H.), HanAll Biopharma (A.D.P.), Glaukos (M.F.), International Keratoconus Academy (J.S.H.), Gas Permeable Lens Institute (J.S.H.), Johnson & Johnson Vision (J.S.H.), Tarsus (J.S.H.), and Metro Optics (J.S.H.). Dr Pucker is an employee of Lexitas Pharma Services and owns a consulting service (Eminent Ophthalmic Services, LLC), although neither of these positions pose a conflict of interest to the current work. Dr Malooley has no conflicts of interest to report.