_slit-lamp_photograph_of_the_right_eye_revealing_multiple_foreign_bodies_(locations_sho.tiff)
INTRODUCTION
Phacoemulsification cataract extraction surgery with intraocular lens implantation is the most common eye surgery.1 As such, many of the potential complications of this operation are well-known, including posterior capsule rupture and vitreous loss, inflammation, cystoid macular edema, endophthalmitis, and posterior capsular opacification.2 However, intraocular metallic foreign bodies resulting from cataract surgery are rarely described. When presented with this finding, a clinician may wonder how such bodies came to be in the eye, whether they might produce inflammation or toxicity, whether they should be removed, and whether the patient can safely undergo future magnetic resonance imaging. To explore these questions, this case report presents a patient with multiple retained intraocular metallic foreign bodies after phacoemulsification and reviews the literature on the subject. No identifiable health information was included in this case report.
CASE REPORT
An 88-year-old White man presented for routine eyecare after cataract extraction of the right eye performed approximately 1 month prior at another office. The patient reported no surgical or postoperative complications of the procedure. Medical and surgical records of past eyecare were neither available nor later obtained.
Aside from bilateral cataract extraction, the patient’s ocular history was otherwise unremarkable. His medical history was significant for coronary atherosclerosis, hypertension, sleep apnea, osteoarthritis, and benign prostatic hyperplasia, for which he had undergone transurethral resection. He took the following medications and supplements: carvedilol, clopidogrel bisulfate, diclofenac topical gel, ezetimibe, hydralazine, isosorbide mononitrate, mirtazapine, pantoprazole, vitamin D3, cranberry extract, cyanocobalamin, and garlic oil. He was allergic or had suffered adverse reactions to amiodarone and omeprazole.
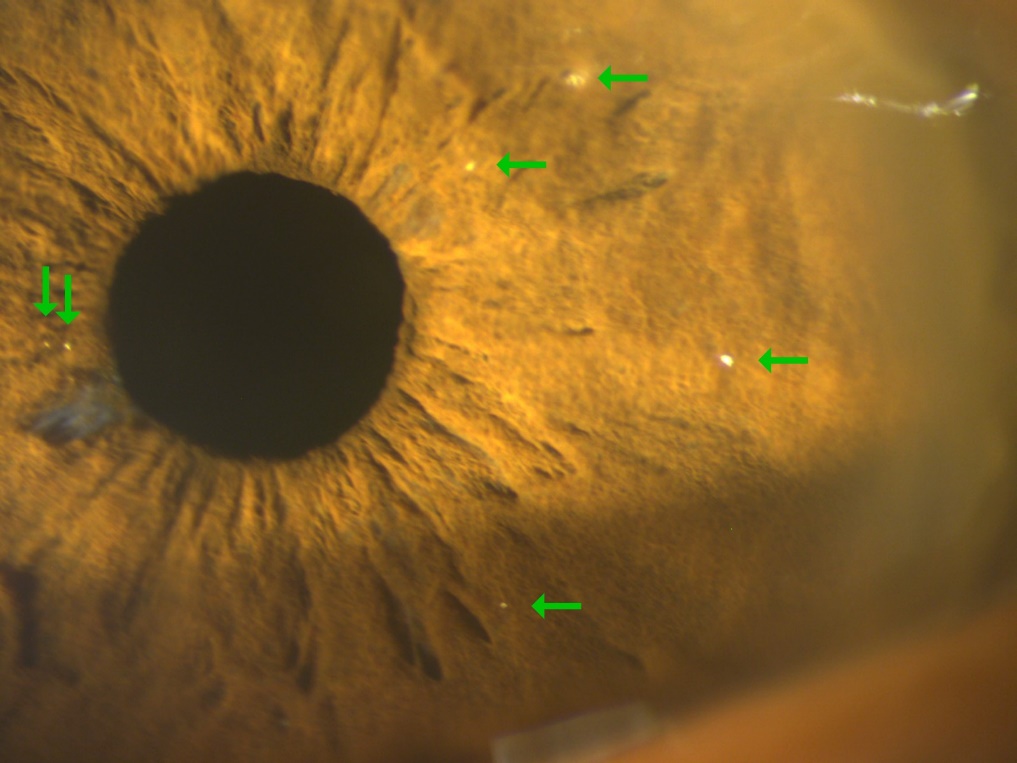
Best-corrected visual acuity was 20/20-2 in the right eye and 20/25+2 in the left. Intraocular pressure was 9 mm Hg in the right eye and 12 mm Hg in the left eye by rebound tonometry. Pupil testing, extraocular motility, and confrontation visual fields were normal in both eyes. Slit-lamp biomicroscopy revealed dozens of refractile, metallic-appearing foreign bodies of various sizes embedded in the temporal incision tunnel and superior paracentesis site of the right cornea at various depths (Figure 1). There were no rust rings. Approximately 7 to 9 similar foreign bodies were embedded in the right iris stroma in a nonspecific pattern (Figure 2). The largest of these foreign bodies was less than 0.5 mm in diameter. There was a small amount of iris atrophy at the inferotemporal pupil edge. The left cornea was clear and left iris normal except for a small amount of iris atrophy at the superotemporal pupil border. Both anterior chambers were deep and quiet. There were centered posterior chamber intraocular lenses seated in the capsular bag of each eye. No foreign bodies were present on the intraocular lenses or within the anterior or posterior vitreous. Gonioscopy of the iridocorneal angle showed a single refractile foreign body on the right iris adjacent to the inferior angle, but both angles themselves were open and clear of any material. Dilated fundus examination showed well-perfused optic nerves with distinct margins. There were intermediate drusen and mild pigment clumping of the retinal pigmented epithelium in each macula but no foreign bodies embedded in the retinas. Optical coherence tomography showed no macular edema or choroidal neovascular membranes in either eye. All other examination findings were normal.
_slit-lamp_photograph_of_the_right_eye_revealing_multiple_foreign_bodies_(locations_sho.tiff)

The presence of foreign bodies in both the main incision tunnel and superior paracentesis site of the right eye strongly implied a surgical etiology. Additionally, the lack of an additional corneal entrance scar from a foreign body argued against the hypothesis that a preexisting intraocular foreign object had been fragmented during the surgery. The patient was diagnosed with moderate dry age-related macular degeneration in both eyes and intraocular metallic foreign bodies after phacoemulsification in the right eye. He was educated in preventive measures to reduce the risk for macular degeneration progression, provided with The Age-Related Eye Disease Study 2 eye vitamins twice a day, and encouraged to perform Amsler grid home monitoring. Because he was unconcerned to learn that he had retained intraocular metallic foreign bodies and because they appeared inert, these were observed and remained unchanged over 2 years of follow-up.
DISCUSSION
No reliable assessment exists regarding the prevalence of intraocular metallic foreign bodies after phacoemulsification.3 Because their diagnosis is often trivial, studies have instead focused on identifying their origin. Historically, various sources have been proposed, including the following: touch of the phaco tip with a second instrument,4 cavitation erosion of the phaco needle surface,5 and annealed fragments shaken loose from the phaco tip.6 Given the diversity of surgical environments and instruments across the world since the inception of phacoemulsification, it is perhaps too simplistic to assume that all intraocular metallic foreign bodies resulting from this procedure always possess the exact same origin. For example, Arbisser described particulates introduced into the eye during cataract surgery that were examined by the manufacturer via scanning electron microscopy.7 These were identified as silver matching the blazing on the phaco handpiece shell. She also stated that the manufacturer had identified copper particulate in other cases, the presumed origin of which was plumbing that contaminated the water used in local autoclaves. In contrast, Chaudhari et al reported that by using scanning electron microscopy, they had matched intraocular metallic foreign bodies introduced intraoperatively to the inner surface of the wrench used to tighten their phaco needles.8 Notably, not all intraocular metallic foreign bodies introduced during cataract surgery are small enough to pose such a diagnostic challenge. There are also reports of fractured phaco tips,9,10 the broken off head of a lens-manipulating instrument,11 and surgical needles located in eyes after phacoemulsification.12,13 In our patient, the high number of intraocular metallic foreign bodies present in both surgical wounds of a single eye implicates the phaco handpiece, which is the most commonly suspected source of metal particles after cataract surgery.3
Although intraocular metallic foreign bodies introduced during phacoemulsification are generally described as inert,3 various metals do produce toxic sequelae within the eye. For example, the effects of iron and copper are well-documented, causing ocular siderosis or chalcosis, respectively.14–16 As such, there are cases of intraocular metallic foreign bodies after phacoemulsification that were not inert. Stangos et al reported a 1.6-mm × 0.4-mm intraocular metallic foreign body composed of copper, aluminum, and zinc embedded in the iris after cataract surgery that caused chronic recalcitrant inflammation, which resolved after its removal.17 Presumably, the foreign body’s copper content bore primary responsibility for inciting a vigorous ocular response. Zacks et al detailed a retained surgical needle of unknown composition in the anterior chamber associated with inflammatory corneal endothelial deposits as well as ongoing chronic cystoid macular edema.12 However, in this case, there was an anterior chamber intraocular lens in the eye, which can also cause inflammation.18
Determining the composition of an intraocular metallic foreign body after cataract surgery can be a challenge. Although the color and reflectivity of the metal may provide some clues, surface coatings or alloys composed of multiple metals might produce diagnostic uncertainty. A systematic evaluation of items in the surgical field coupled with manufacturer-supplied data on instrument composition can be undertaken.3 As mentioned earlier, several authors matched foreign bodies extracted from the eye to surgical instruments via scanning electron microscopy.7,8 Additional information can be gleaned from the ocular response to the metal; if the foreign body is causing inflammation, then it likely has a component known to do so. Lastly, chemical analysis of aqueous humor containing foreign body fragments can be employed.17
Traditionally, the decision to remove intraocular metallic foreign bodies is informed by the risks of leaving them in place weighed against the risks of extraction in a dialogue between the patient and the surgeon. If an intraocular metallic foreign body produces uncontrollable inflammation or is known to be toxic to ocular tissue, the conversation may be relatively straightforward. One often overlooked factor in the eyecare literature, however, is the patient’s perspective. Given that each patient is a unique person with individual needs and contexts, a greater emphasis on incorporating patient preferences has been proposed, in part to address ethical considerations in cases where clinicians make medical decisions without adequate patient input.19 Deemed “shared decision-making,” this collaborative process between patients and clinicians integrates patient goals and values with clinician experience and evidence-based medicine. It has been reported that patients and surgeons generally express a preference toward an egalitarian approach.20 Consequentially, although a particular foreign body may or may not necessitate removal from a strict ophthalmic perspective, it is worthwhile to incorporate the patient’s preferences into surgical decision-making. Thus, in some circumstances, it may be appropriate to remove an intraocular foreign body even when it is thought to be inert.
Extraction of intraocular metallic foreign bodies after phacoemulsification can be accomplished via a return to the operating room. The individual characteristics of the case inform the surgical approach. In general, limbal incision techniques and sterile forceps are employed.3 Importantly, it may be challenging to access and remove a multitude of tiny fragments as seen in this case.
The specific composition of retained intraocular metallic fragments has implications for magnetic resonance imaging. Ferromagnetic metals, such as iron, nickel, cobalt, and their alloys, can migrate or rotate under the influence of magnetic resonance scanners, inflicting mechanical trauma to the surrounding tissue.21 Reported ocular sequelae of such an event include pain,22 hyphema,21,23 cataract,24 and vitreous hemorrhage.25 The gradient magnetic fields of magnetic resonance scanners can also induce an electric current, especially in wires or loops, which can heat the metal and produce burns.26 For these reasons, among others, computed tomography remains the gold standard for evaluating suspected intraorbital foreign bodies and can be employed as a screening tool before magnetic resonance imaging.27 Notably, in 2013, the American College of Radiology recommended that any patient with a history of orbital trauma by a potential ferromagnetic foreign object for which they sought medical care must have their orbits cleared via imaging before undergoing magnetic resonance imaging.26 With respect to ophthalmic surgical instruments, any specific grade of surgical steel may or may not be magnetic, depending on its individual iron content, whereas the titanium found in phaco tips is not.28
The size of a ferromagnetic foreign body also influences its potential for movement. Rabbit model studies have demonstrated that periocular and intraocular foreign bodies smaller than 3 × 1 × 1 mm do not move when exposed to a 2-T-strength magnetic resonance magnet.29 Zhang et al reported 2 patients with vitreal ferromagnetic foreign bodies less than or equal to 0.5 mm that underwent 1-T-strength magnetic resonance imaging without apparent ocular sequelae.30 (For reference, most commercial magnetic resonance scanners currently employ static magnetic fields of 1.5 T or 3 T, but ultrahigh magnetic fields equal to or greater than 7 T might become more prevalent outside of research.)31 These papers suggest that our patient’s less than 0.5-mm foreign bodies are unlikely to move if exposed to regular strength magnetic resonance magnets, even if the foreign bodies were highly ferromagnetic. However, screening computed tomography before magnetic resonance imaging could be reassuring and serve to rule out the presence of a larger foreign body that went undetected on clinical examination.
CONCLUSION
Metallic foreign bodies that enter the eye during cataract surgery may originate from diverse sources. Most of these foreign bodies are inert, but some can cause inflammation or toxicity or create a contraindication for future magnetic resonance studies. The exact risks depend on the metal’s size, shape, composition, and ferromagnetic qualities. Consequently, careful examination and consideration is prudent when intraocular metallic foreign bodies are detected.
TAKE HOME POINTS
-
Different cases of intraocular metallic foreign bodies after phacoemulsification do not necessarily share the same metallic source.
-
Most, but not all, intraocular metallic foreign bodies after phacoemulsification are inert.
-
When contemplating the removal of an intraocular metallic foreign body, shared decision-making integrates the patient’s goals, values, and preferences into medical decisions instead of relying solely on ophthalmic indications.
-
Intraocular metallic foreign body risk factors for magnetic resonance imaging include ferromagnetic composition (such as iron, nickel, and cobalt levels) and size equal to or greater than 3 × 1 × 1 mm when exposed to 2 T.