

INTRODUCTION
Chronic myeloid leukemia is a type of cancer that originates in the bone marrow and is characterized by uncontrolled growth of myeloid white blood cells.1 The underlying cause of chronic myeloid leukemia is a genetic mutation in the Philadelphia chromosome that is caused by a translocation between chromosome 9 and 22.1 This translocation creates a gene sequence called BCR-ABL1, which produces a protein with abnormal tyrosine kinase activity that causes an increase in the proliferation of myeloid cells.1 There are 3 phases of chronic myeloid leukemia:
-
The chronic phase is the initial stage in which the disease progresses slowly.1–3 Most patients are asymptomatic or have mild symptoms of fatigue, weight loss, and abdominal discomfort, and at this point, the white blood cells function relatively normally.1–3
-
The accelerated phase is the intermediate stage in which the disease progresses rapidly with worsening symptoms such as increased fatigue, fever, bone pain, and spleen enlargement.3 The number of immature white blood cells (blasts) in the bone marrow and blood increases in this phase.1–3
-
The last phase is the blast crisis in which the number of immature blast cells increases significantly and results in the crowding out of normal blood cells. This resembles acute leukemia and requires urgent treatment.1–3
Targeted therapies have been created, such as the tyrosine kinase inhibitor imatinib mesylate, which was the first US Food and Drug Administration–approved tyrosine kinase inhibitor in 2001 for chronic myeloid leukemia.3 It is an oral chemotherapeutic designed to target the BCR-ABL1 hybrid protein, a tyrosine kinase inhibitor protein produced in patients with Philadelphia chromosome–positive chronic myeloid leukemia.1–3 As one of the first novel treatments for chronic myeloid leukemia, it has a larger side-effect profile than some of the newer medications.3 There are 50 US Food and Drug Administration–approved tyrosine kinase inhibitors with many applications for many different cancers, but we will be focusing on those used to treat chronic myeloid leukemia.2,3 There are 4 different stages of treatment milestones for patients with chronic myeloid leukemia: early molecular response, complete cytogenic response, major molecular response, and deep molecular remission.4 Early molecular response occurs when BCR-ABL1 transcripts are measured at less than 10% at 3 months and 6 months after starting tyrosine kinase inhibitors. This predicts the likelihood that a patient will respond to treatment long-term.4 The next treatment milestone is called complete cytogenetic response. This is defined as the absence of the Philadelphia chromosome in bone marrow, which is equal to a BCR-ABL1 level of 0.1% to 1% and is ideally achieved within 12 to 18 months after starting treatment.4 Major molecular response is the next milestone, where patients have a BCR-ABL1 level of less than 0.1%.4 The final stage is deep molecular remission, which is a value less than 0.0032% of the BCR-ABL1 gene for at least 2 years to consider stopping tyrosine kinase inhibitor treatment.4
Treatment-free remission is achieved when a patient who has discontinued tyrosine kinase inhibitor therapy maintains a deep molecular remission and does not need to restart treatment.4–6 The discontinuation of tyrosine kinase treatment happens to 40% to 60% of patients with chronic myeloid leukemia with long-term deep molecular response. The discontinuation of treatment is varied for every patient based on their BCR-ABL1 gene values when measured through quantitative polymerase chain reaction.4–6 Treatment goals for patients with chronic myeloid leukemia are complete hematologic, cytogenic, and molecular remission for the best possible long-term outcome.6,7
The case presented will highlight the importance of external examination of patients presenting with advanced dry eye disease. The patient presented with new signs of periorbital edema, which is a known side effect of imatinib mesylate, a first-generation tyrosine kinase inhibitor used to treat chronic myeloid leukemia with concurrent worsening aqueous deficient dry eye. This case will review how optometrists fit into this type of medical management of patients.

CASE REPORT
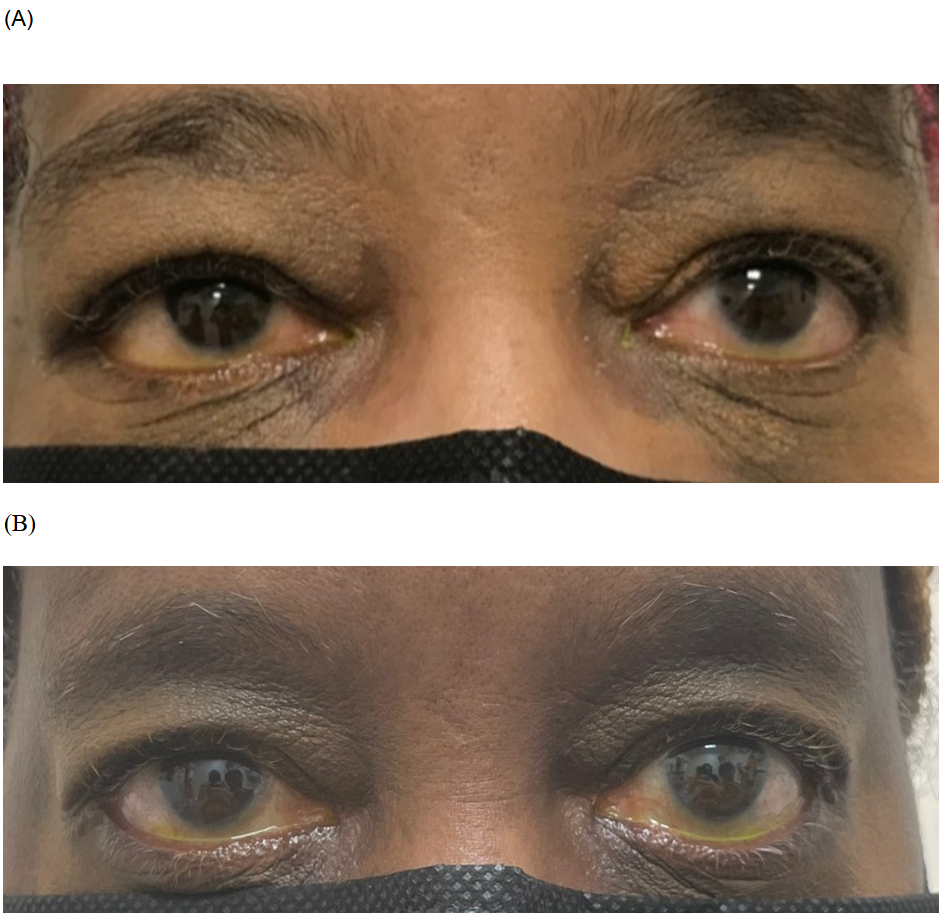
A 64-year-old black woman presented to our clinic with complaints of worsening dryness and periorbital swelling. The best-corrected visual acuity with Snellen acuity was 20/20 for the right eye and 20/40 for the left eye. Intraocular pressure was 11 mm Hg and 13 mm Hg in the right and left eye, respectively. Pupils, extraocular motility, and confrontation visual fields were unremarkable. An external examination revealed that the patient had significant greater-than-inferior periorbital swelling of both eyes along with lid edema (Figures 1 and 2) and reported increased swelling at the ankles. Medical history was significant for chronic myeloid leukemia, hyperlipidemia, normal tension glaucoma of both eyes, strabismic amblyopia of the left eye, vertigo with mild headaches, surgical removal of a pituitary adenoma 30 years ago, and sleep apnea. Ocular medications currently used were latanoprost 0.005% ophthalmic solution once a day at night in both eyes, lifitegrast 5% ophthalmic solution twice a day in both eyes, and mineral oil with white petrolatum (REFRESH PM) ointment nightly in both eyes. Systemic treatments currently used were as follows: imatinib mesylate 400-mg tablet taken orally daily (GLEEVEC), a continuous positive air pressure machine, docusate sodium 100-mg tablet taken orally daily, doxycycline hyclate 100-mg tablet taken orally daily, metronidazole 250-mg tablet taken orally daily, and rosuvastatin 10-mg tablet taken orally daily. The patient had no history of allogenous hematopoietic stem cell transplantation to manage chronic myeloid leukemia and was in deep molecular response remission with tyrosine kinase inhibitor use. It was recommended to the patient to add cold compresses to her face once daily in the morning to help reduce swelling. A follow-up examination was scheduled in 3 months to re-evaluate the periorbital edema and to discuss these new signs and symptoms with her oncologist and nephrologist to determine whether medication changes were necessary.
_initial_present.png)
_initial_presentation_vs_(b)_th.png)
At the follow-up examination, the best-corrected visual acuity was stable from the previous examination. The patient reported improving symptoms of dryness with continued lifitegrast 5% ophthalmic solution instilled twice a day in both eyes, mineral oil with white petrolatum ointment used daily at night, and the daily use of cold compresses. The patient’s oncologist changed her chronic myeloid leukemia treatment to bosutinib, a second-generation tyrosine kinase inhibitor, and recommended increasing the intake of electrolytes and water consumption. This resulted in improved signs of periorbital and lid edema (Figures 1 and 2). The patient is being monitored every 3 months to manage for any signs of worsening dry eye symptoms or signs of a recurrence of periorbital edema.
DISCUSSION
Imatinib mesylate is a BCR-ABL1 tyrosine kinase inhibitor for the treatment of Philadelphia chromosome chronic myeloid leukemia.5 Tyrosine kinase inhibitors are a first-line medication for chronic myeloid leukemia and have known ocular and systemic side effects, which include periorbital edema, muscle cramps, skin rashes, and significant epiphora.5,6 When patients are examined, it is important to rule out other causes of periorbital edema such as kidney disease, thyroid disease, periorbital cellulitis, and many others.5,6 This highlights the value of a thorough case history and learning the ocular side effects of new cancer medications. The goal of tyrosine kinase inhibitors is to block receptor tyrosine kinases from modifying cell growth, migration, differentiation, apoptosis, and death in tyrosine kinases that are mutated or dysfunctional.5–7 In chronic myeloid leukemia, the goal is to prevent the production of BCR-ABL1 protein, which would cause a dysfunctional nonmature myeloid cell to form a blast cell.5–8 There are currently 4 tyrosine kinase inhibitors that are second-generation and third-generation treatments for chronic myeloid leukemia: ponatinib (ICLUSIG), bosutinib (BOSULIF), nilotinib (TASIGNA), and dasatinib (SPRYCEL). All the treatments have similar side-effect profiles; however, the incidence of periorbital swelling is higher with imatinib, a first-generation tyrosine kinase inhibitor.5–10 The second-generation tyrosine kinase inhibitors indicated for chronic myeloid leukemia (bosutinib, dasatinib, nilotinib, ponatinib) have comparable survival results to imatinib.10 In a German chronic myeloid leukemia trial of 1551 subjects, only 26.5% of patients treated with imatinib were changed to second-generation tyrosine kinase inhibitors; 10% were due to resistance and the others to toxicities/other reasons.10 A patient is monitored by evaluating BCR-ABL1 transcripts to determine the status of their chronic myeloid leukemia and whether treatment is working. The percentage of transcripts should decrease over time, leading to a state of treatment-free remission.10 Sometimes patients develop resistance to tyrosine kinase inhibitors and the medication is not as effective in preventing the production of the BCR-ABL1 gene, which is another consideration relevant for switching to a different tyrosine kinase inhibitor.10
Monitoring for potential ocular side effects such as periorbital edema and concurrent dry eye management in the case of our patient is important for optometrists. Other common ocular side effects of tyrosine kinase inhibitors are central serous chorioretinopathy, pigment epithelial detachments, and keratitis.5,6 Keratitis can develop because of the slowing of regeneration of epithelial cells, leading to delayed healing and possibly scarring.5,6 The following describes other side effects associated with tyrosine kinase inhibitors:
-
The side effects of imatinib include rashes, fluid retention, edema, weight gain, musculoskeletal aches, diarrhea, skin depigmentation, and possible renal toxicity.5,6
-
The effects of nilotinib include rashes, headaches, an increase in bilirubin, impaired glycemic control, dyslipidemia along with renal toxicity, pancreatitis, and worsening diabetes.5
-
The side effects of dasatinib include pleural effusion, cytopenia with pulmonary hypertension, and systemic hypertension.5
-
The side effects of bosutinib include gastrointestinal toxicity (diarrhea/colitis), renal dysfunction, liver dysfunction, and enterocolitis.5
-
The side effects of ponatinib include rash, hypertension, and pancreatitis along with hepatic toxicity.5
Periorbital swelling is occasionally the presenting sign of kidney disease, with additional edema noted at the ankles and legs.9,11 Other clinical signs consistent with kidney disease are elevated blood pressure and weight gain.9,11 Patients with chronic myeloid leukemia normally presented with weight loss owing to the medication use.9,11 The periorbital edema can be reduced with conservative management, such as observing a low-sodium diet, restricting fluid intake, elevating the head while sleeping, and taking diuretics.9,11
Invasive treatment is necessary for patients without enough of a reduction of their BCR-ABL1 transcript levels when treated with tyrosine kinase inhibitors. The next available treatment is an allogeneic hematopoietic stem cell transplant.12,13 The transplant involves having the patient’s stem and cancer cells destroyed with ablative radiation and chemotherapy to make their bone marrow empty, then administering the bone marrow transplant to allow new T-cell lymphocytes to circulate throughout the body from the graft.12,13 A common complication after an allogeneic hematopoietic stem cell transplant is the development of graft-versus-host disease.12,13 Graft-versus-host disease occurs when immunocompetent T-cell lymphocytes in the transplanted graft attack the immunodeficient host tissue owing to inadequate histocompatibility.12,13 This usually occurs within 100 days after hematopoietic stem cell transplant, causing tissue damage to the host’s body.12,13 There are 4 main classifications of graft-versus-host disease: acute classic, late-onset, classic, and overlap syndrome.12,13 Acute classic graft-versus-host disease occurs within 100 days after the hematopoietic stem cell transplant, whereas late-onset graft-versus-host disease has the same clinical features as acute classic graft-versus-host disease but occurs 100 days after hematopoietic stem cell transplant.12,13 Classic chronic graft-versus-host disease presents after 100 days with the classic features of graft-versus-host disease.12,13 Overlap syndrome occurs at any time after transplantation with acute and chronic features.12,13
The clinical presentation of acute graft-versus-host disease usually affects the skin, gastrointestinal tract, and liver and also can affect the lungs, kidneys, and eyes.12–14 Chronic graft-versus-host disease has several similar features in common with collagen vascular disorders and systemic sclerosis such as scleroderma and Sjogren syndrome.12–15 Patients are placed on prophylactic treatment for graft-versus-host disease after hematopoietic stem cell transplant; the most common regimen includes a combination of cyclosporine-A and methotrexate for several months after hematopoietic stem cell transplant.12–15 Graft-versus-host disease can affect the ocular surface, causing severe dry eye disease. This can be managed with treatments such as cyclosporine 0.05% ophthalmic emulsion, cyclosporine 0.09% ophthalmic solution (CEQUA), cyclosporine 0.1% ophthalmic solution (VEVYE), and lifitegrast 5% ophthalmic solution.15 One particular treatment that has shown significant improvement in managing the signs and symptoms of ocular surface disease in patients with chronic graft-versus-host disease is autologous serum tears, which are created from extracting patients’ blood and separating liquid and cellular components to create nutrient- and growth factor–rich tears.14–16
CONCLUSION
In conclusion, chronic myeloid leukemia is a complex disease for which first-line treatment involves tyrosine kinase inhibitors such as imatinib by specifically targeting the underlying molecular abnormalities. However, the medications can cause side effects such as periorbital edema and ocular surface disease. This case report highlights the importance of recognizing and managing these side effects as eyecare providers and of collaborating with other health care providers to optimize these patients’ care. Optometrists are an active part of the medical management of patients, and knowing the ocular side effects of new cancer medications is crucial to improving patients’ overall well-being during their treatment process.
TAKE HOME POINTS
-
Tyrosine kinase inhibitors are a first-line chemotherapeutic treatment for chronic myeloid leukemia. Patients can present with side effects such as periorbital edema. Increasing electrolyte intake, along with cold compress use, and consulting with hematology and oncology to discuss new findings will enhance the quality of care for these patients.
-
Knowing the ocular side effects of cancer medications is important for optometrists as primary eyecare providers.
-
Determine whether a patient with chronic myeloid leukemia has received an allogeneic hematopoietic stem cell transplant and whether they have developed graft-versus-host disease to determine the appropriate management for their dry eye symptoms.
-
Using ocular medications with anti-inflammatory properties such as cyclosporine 0.05%, 0.09%, or 0.1% or lifitegrast 5% should be part of first-line dry eye treatment in patients with chronic myeloid leukemia.
No identifiable health information was included in this case report.