INTRODUCTION
Choroidal folds are undulations involving Bruch’s membrane, the inner choroid, and often the outer retina that appear as striations of alternating dark and light bands under fundoscopic examination.1,2 When the folds also involve the inner retina, they are described as chorioretinal folds.3,4 Previously, it was thought that the majority of cases were idiopathic in nature; however, with improved diagnostic technology, it is estimated that in only approximately 15% of cases another etiology cannot be found.3 Patients with choroidal and chorioretinal folds can be with or without symptoms depending on etiology and severity. Blurred vision or metamorphopsia are the most common presenting symptoms expressed.5,6
There are a variety of ocular and extraocular etiologies resulting in choroidal and chorioretinal folds delineated in the literature.1,5 The most common causes for monocular cases are scleritis, retinal vascular occlusion, and ocular tumors, whereas macular degeneration, axial hyperopia, and other unknown or idiopathic causes can result in bilateral cases.1,7 Sometimes, these folds can be the only sign of posterior scleritis.8
Upon discovery of choroidal or chorioretinal folds, differential diagnoses should include both ocular and extraocular conditions. Management strategies are largely dependent on etiology and should always involve a thorough workup with appropriate ancillary testing, radiological imaging, and laboratory testing if indicated.5 Serious underlying conditions may be elucidated as a result of this single ocular finding and should be treated appropriately. Idiopathic choroidal or chorioretinal folds is a diagnosis of exclusion and requires regular observation.
This case series aims to review appropriate diagnostic protocol and to discuss differential diagnoses in 2 cases of unilateral chorioretinal folds and 1 case of bilateral choroidal folds with varying degrees of contributing medical history.
CASE SERIES
Case 1
A 45-year-old White man presented for a new patient comprehensive eye examination in 2022 with a chief complaint of recent blur to vision greater at night and difficulty focusing at near. He linked some of his vision problems with personal history of traumatic brain injury in 2009. Ocular history was remarkable for dry eye syndrome and a foreign body removal of the left eye. Medical history was significant for traumatic brain injury from multiple blast exposures while in military service in 2003, 2005, and 2008 without loss of consciousness, irritable bowel syndrome, post-traumatic-stress disorder, and migraine. For these conditions he was taking artificial tears, baclofen, capsaicin cream, famotidine, lactobacillus, meloxicam, and sumatriptan.
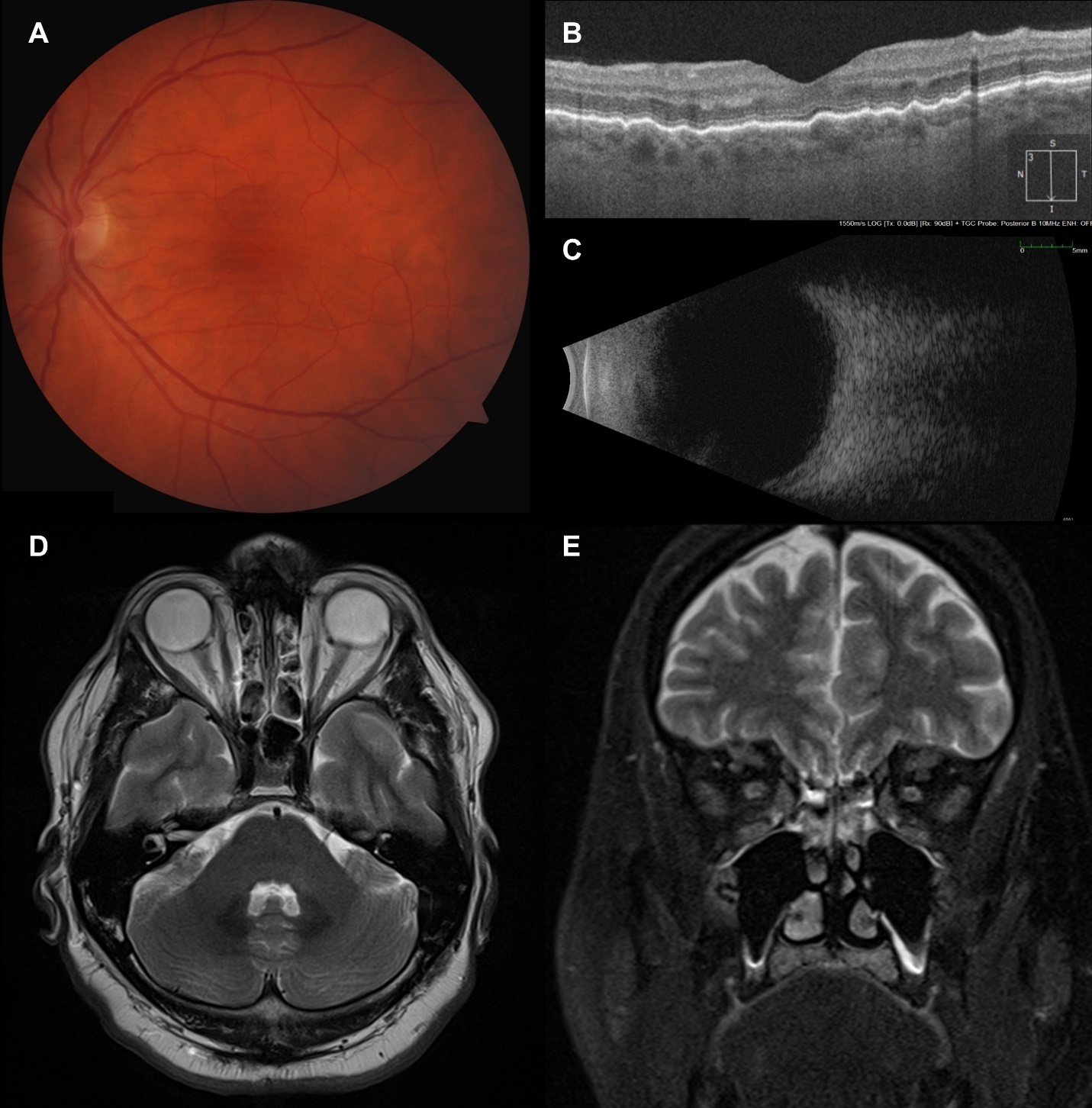
Best-corrected visual acuities were 20/20 in each eye with a mild hyperopic refractive error of +0.25 diopter sphere in the right eye and +1.00 -0.25 × 095 in the left eye. Pupils were equally round and reactive to light without an afferent pupillary defect. Slit lamp examination revealed mild meibomian gland inspissation and telangiectasia of the upper and lower eyelid margins bilaterally but was otherwise unremarkable with no signs of anterior segment inflammation. Intraocular pressures by Goldmann applanation tonometry were 16 mmHg in the right eye and 18 mmHg in the left eye. Dilated funduscopic examination demonstrated an absence of disc edema in either eye and diffuse parallel horizontal chorioretinal folds in the macula most prominent nasally toward the optic nerve head in the left eye (Figure 1A). Traditional horizontally oriented optical coherence tomography of the left eye demonstrated mild inner-retinal undulations with mild irregularity of foveal contour, an intact ellipsoid zone, and an absence of frank retinal or choroidal folds (Figure 1B). A vertically oriented 21-line raster optical coherence tomography image, however, revealed diffuse retinal and choroidal undulations in the left eye (Figure 1C). The B-scan ultrasonography demonstrated an average scleral thickness without evidence to support subclinical scleritis (i.e., a T-sign). Axial length was 23.10 mm in the right eye and 22.48 mm in the left eye. Without evidence of possible etiology for the chorioretinal folds in the left eye, magnetic resonance imaging with and without contrast of the brain and orbits was ordered. This imaging ruled out the presence of an ocular or orbital tumor as well as evidence of extraocular muscle thickening that would typically be associated with thyroid eye disease (Figures 1D and 1E).
_color_fundus_photography_of_the_left_eye_demonstrating_horizontal_paral.jpeg)
This patient had mild hyperopia of the eye in question and a systemic diagnosis of irritable bowel syndrome without any sign of ocular inflammation. This patient also has a notable history of head trauma with multiple traumatic brain injuries occurring to the left side of his head. It is possible the history of irritable bowel syndrome could have resulted in past episodes of inflammation like scleritis causing the observed folds. It could also be possible that the previous head trauma could have caused papilledema resulting in the chorioretinal folds. The patient was diagnosed with likely idiopathic chorioretinal folds in the left eye in the context of left-sided head trauma and mild hyperopia in the left eye without significant asymmetry in axial length. In the absence of apparent pathology, the patient was monitored in 3-month intervals without changes to the ocular findings.
Case 2
A 49-year-old White man presented for a comprehensive eye examination as an established patient in 2022 with a chief complaint of blurry vision at distance for a few months with his habitual spectacles. Ocular history was remarkable for congenital cataracts and a welder’s flash arc injury of the left eye. Medical history was significant for renal cell carcinoma with partial right nephrectomy in 2021, chronic kidney disease, abnormal liver function, gastroesophageal reflux disease, and allergic rhinitis. For these conditions he was taking cyanocobalamin, fluticasone, loratadine, and omeprazole.
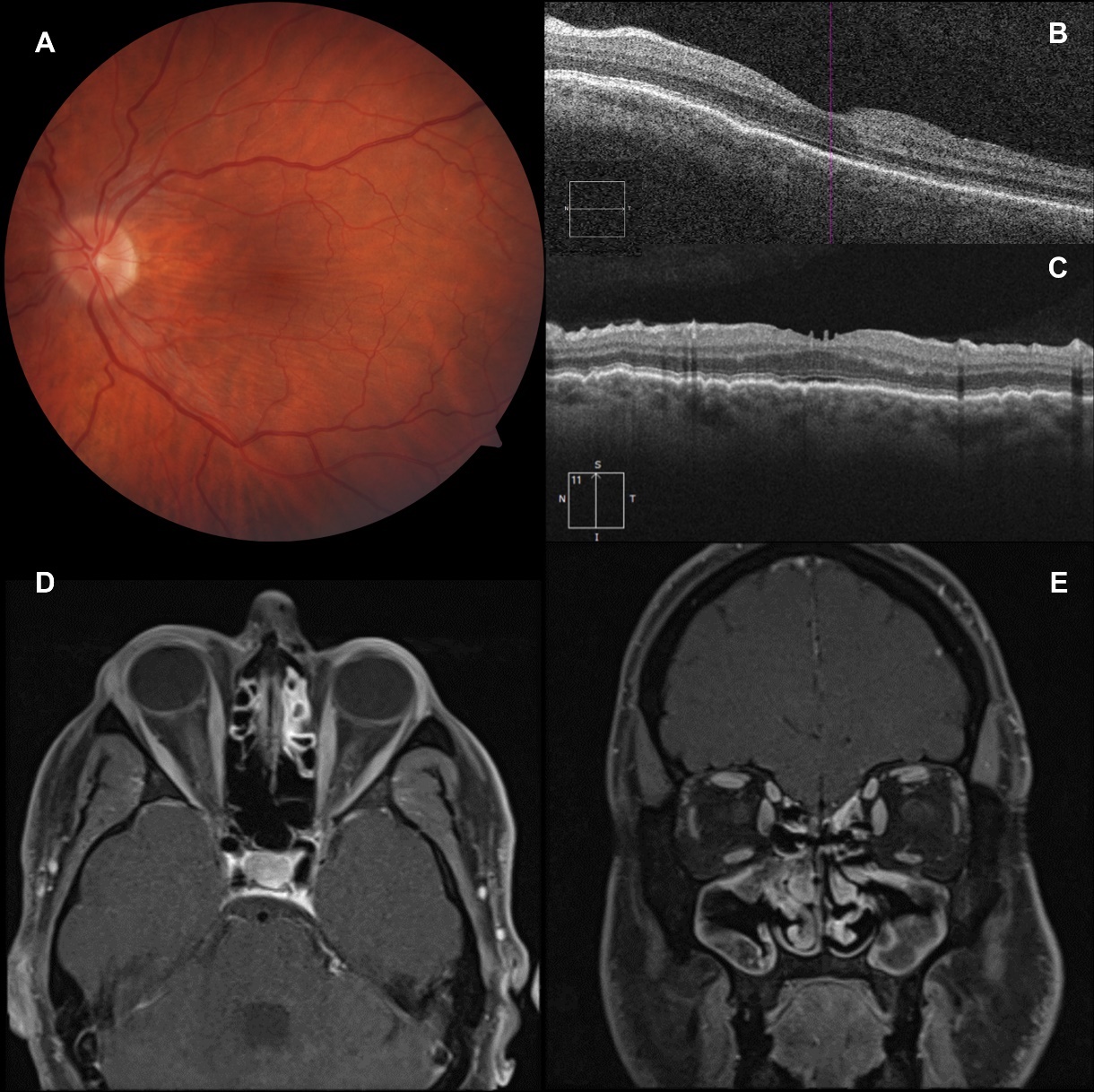
Best-corrected visual acuities were 20/20 in the right eye and 20/20 in the left eye with a mild refractive error of -0.50 -0.25 × 095 in the right eye and +0.75 diopter sphere in the left eye, a hyperopic shift in the left eye compared with his habitual prescription of -0.50 diopter sphere in the right eye and +0.25 diopter sphere in the left eye. Pupils were equally round and reactive to light without an afferent pupillary defect. Slit lamp examination revealed signs of bilateral blepharitis without signs of anterior segment inflammation. Intraocular pressures by iCare tonometry were 14 mmHg in each eye. Dilated funduscopic examination demonstrated an absence of disc edema in either eye and diffuse parallel horizontal chorioretinal folds in the macula in the left eye (Figure 2A). Traditional horizontally oriented optical coherence tomography in the left eye demonstrated mild irregularity of foveal contour, an intact ellipsoid zone, and an absence of retinal or choroidal folds. Vertically oriented optical coherence tomography with enhanced depth imaging demonstrated clear chorioretinal undulations without obvious pathology in the choroid in the left eye (Figure 2B). B-scan ultrasonography showed a moderately thick choroidal appearance in both eyes without intraocular mass or pathology in the left eye (Figure 2C). Magnetic resonance imaging of the orbits revealed an absence of space-occupying lesion or extrinsic optic nerve compression (Figures 2D and 2E). Axial length was measured without significant asymmetry between the eyes: 23.13 mm in the right eye and 22.63 mm in the left eye. Without frank pathology, this patient was diagnosed with unilateral chorioretinal folds of the left eye in the context of acquired unilateral hyperopia of the left eye. An acquired unilateral hyperopic shift should warrant suspicion for unilateral ocular pathology, such as a compressive tumor. In this case, ultrasonography and magnetic resonance imaging ruled out these ocular pathologies. Ocular findings remained stable over interval follow-up examinations.
_color_fundus_photography_of_the_left_eye_showing_horizontal_parallel_ch.jpeg)
Case 3
A 94-year-old White man presented for a new patient comprehensive eye examination in 2017 with a chief complaint of blurry vision while watching television for a few months with his habitual spectacles. Ocular history was remarkable for optic atrophy in the right eye secondary to head trauma with subsequent bilateral papilledema due to subdural hematoma and blood drain in 2013, cataract extraction in both eyes, yttrium-aluminum-garnet laser capsulotomy for posterior subcapsular opacification in both eyes, dry eye syndrome in both eyes, and small retinal hole with laser repair in the left eye. Medical history was significant for hyperlipidemia, hypertension, and gout. For these conditions he was taking allopurinol, glucosamine, lisinopril, and simvastatin.
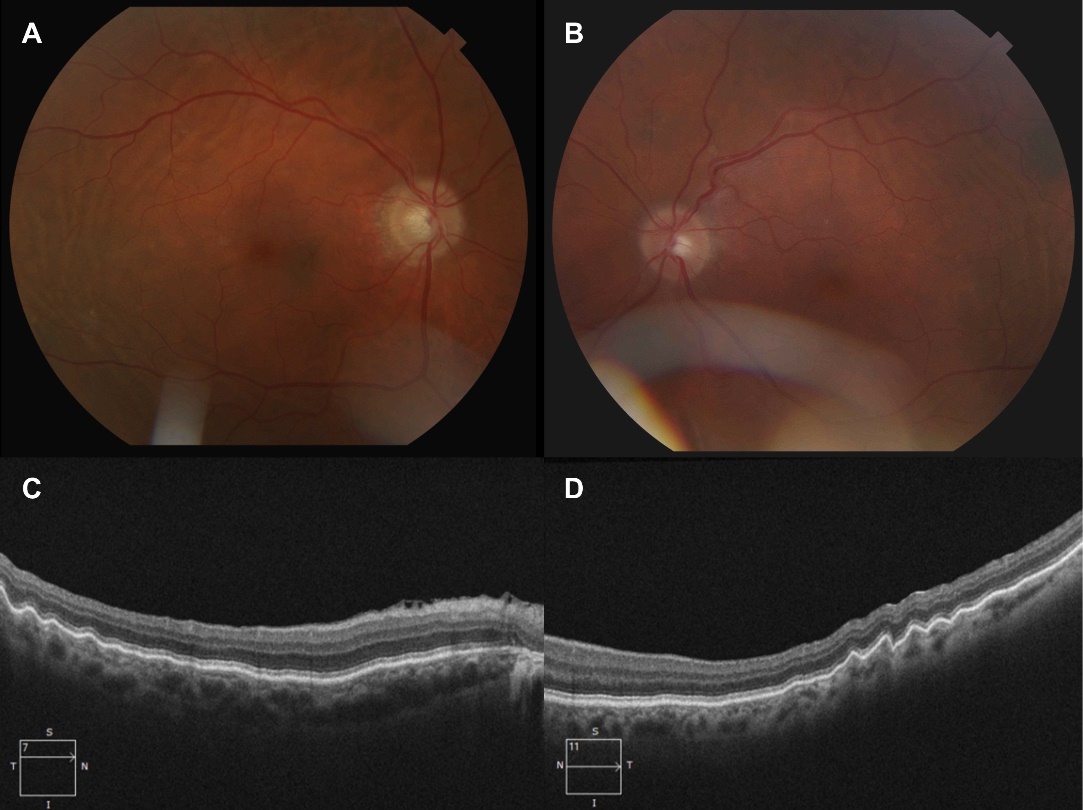
Best-corrected visual acuities were 20/25+1 in the right eye and 20/25+2 in the left eye with a refractive error of +0.75 -1.25 × 101 in the right eye and plano -1.00 × 047 left eye. Pupils were equally round and reactive to light with a 1+ afferent pupillary defect in the right eye. Slit lamp examination revealed posterior chamber intraocular lenses in both eyes and no signs of anterior segment inflammation. Intraocular pressures by Goldmann applanation tonometry were 20 mmHg in each eye. Dilated funduscopic examination revealed concentric choroidal folds temporal to the macula extending superior to inferior in both eyes (Figures 3A and 3B). There were also choroidal nevi present in both eyes, stable optic atrophy in the right eye, and an old retinal hole status post laser repair in the left eye. There was no active disc edema in either eye. Optical coherence tomography 21-line raster over the choroidal folds in each eye demonstrated diffuse outer-retinal and choroidal undulations without obvious pathology within the choroid and an intact ellipsoid zone in each eye (Figures 3C and 3D). Based on his presenting history of head trauma with subdural hematoma causing bilateral papilledema, additional workup was not deemed necessary. Ocular findings remained stable over interval follow-up examinations.
_color_fundus_photography_of_the_right_eye_and_(b)_left_eye_showing_conc.jpeg)
DISCUSSION
Patients with chorioretinal folds may be asymptomatic or may complain of visual disturbances, such as decreased visual acuity or metamorphopsia.1–3,9 These folds are commonly parallel to one another in horizontal or vertical orientation but have also been observed in radiating or concentric patterns.9,10 They tend to be limited to the posterior pole and can be unilateral or bilateral.2 The exact pathophysiology is not clearly understood but may be attributed to changes between the attachment of Bruch’s membrane under the retinal pigment epithelial layer and congestion in the choriocapillaris.2 Choroidal folds are thought to develop as a result of any condition causing a reduction of the inner surface of the sclera, such as scleral thickening or shrinkage, resulting in a buckling force affecting the inner choroid, including Bruch’s membrane, the overlying retinal pigmented epithelium, and the outer retinal layer.4,6 When this buckling also results in retinal undulations, the findings are described as chorioretinal folds.9 It should also be mentioned that this force must exceed that of the force intraocular pressure exerts on the choroid.4,11 This phenomenon is to be differentiated from a simple indentation of the sclera from an outside force, which alone does not result in chorioretinal folds.1 There are currently no prevalence statistics on chorioretinal folds within the general public. No evidence exists to suggest a genetic component to development of chorioretinal folds.1
Upon discovery of chorioretinal folds, differential diagnoses should include such ocular conditions as choroidal tumor, idiopathic orbital inflammatory syndrome, posterior scleritis, hypotony, retinal detachment, hyperopia, scleral laceration, papilledema, postoperative sequelae, choroidal neovascular membranes, central serous chorioretinopathy, and uveal effusion syndrome.1,7,10 Extraocular diagnoses can include orbital tumors, thyroid eye disease, frontoethmoidal mucoceles, intracranial hypertension without evidence of papilledema, meningioma, inflammatory bowel disease, Lyme disease, systemic autoimmune disorders such as rheumatoid arthritis and systemic lupus erythematous, scleral buckle, or radiotherapy plaques and trauma.1,12
The bilateral clinical findings in case 3 are attributable to the patient’s history of head trauma with bilateral subdural hematoma, which resulted in sequential papilledema, optic atrophy, and choroidal folds. Significant clinical findings in cases 1 and 2 center primarily around the absence of findings. The presence of unilateral chorioretinal folds led to ordering several additional ancillary and radiological tests, all of which demonstrated normal results without revealing possible etiology for fundoscopic findings. Without evidence for causal pathology leading to the development of chorioretinal folds as in case 1, an idiopathic etiological label can be assigned to be updated if warranted at future follow-up. Case 2 did demonstrate a mild hyperopic shift of the eye of interest, which could explain the findings.
The imaging studies used in the diagnosis of these patients include fundus photography, fundus autofluorescence, optical coherence tomography, B-scan ultrasonography, fluorescein angiography, measurement of axial length, and magnetic resonance imaging.4,10 Fluorescein angiography accentuates the choroidal folds by increasing the contrast between the peaks and troughs.2,10 Perpendicular orientation of optical coherence tomography imaging to the chorioretinal folds is critical to determine the extent of said finding and in differentiating choroidal folds from chorioretinal folds.4,13 Optical coherence tomography of choroidal folds will be seen as waviness of the retinal pigment epithelium and choroid with a fairly smooth inner retinal surface, whereas imaging of chorioretinal folds will show a full-thickness waviness involving inner retina, retinal pigment epithelium, and choroid.4 Either of these two will be best imaged if the optical coherence tomography obtains perpendicular cross-sectional images. As demonstrated in cases 1 and 2, traditional horizontally oriented images cannot fully capture the horizontally orientated chorioretinal folds as a vertically oriented scan can (Figures 1 and 2). B-scan ultrasonography can rule out the presence of intraocular mass and posterior scleritis.4 Magnetic resonance imaging with and without contrast can rule out thyroid eye disease**,** presence of orbital tumor, meningioma, frontoethmoidal mucoceles, and intracranial hypertension.1 If magnetic resonance imaging was contraindicated, computed tomography imaging could be ordered as a relative substitute. Should the patient demonstrate associated findings such as ocular inflammation, laboratory testing to include complete blood count, erythrocyte sedimentation rate, rheumatoid factor, antinuclear antibody, QuantiFERON Gold, angiotensin-converting enzyme, syphilis antibodies, and human leukocyte antigen B27 can also be indicated to rule in or out a systemic inflammatory or infectious etiology.8 More specific laboratory testing for infectious etiologies such as Lyme disease serology can be indicated depending on a detailed patient case history.
If all other possible etiologies are ruled out via the imaging studies dictated above, the leading differential remains as idiopathic. Close monitoring without intervention is recommended in the absence of treatable pathology. Regression of chorioretinal folds is possible in both bilateral and unilateral cases, within variable time frames, following appropriate treatment when the underlying etiology can be elucidated.4 Prognosis is favorable without the presence of other associated conditions, but complications including secondary choroidal neovascularization have been documented and should be referred and managed appropriately by ophthalmology.14 The use of intravitreal anti–vascular endothelial growth factor injections to treat choroidal neovascularization related to chorioretinal folds has been shown to be effective, although visual acuity outcomes vary.15 Photodynamic therapy and sustained-release dexamethasone implants have also been shown to be effective for treatment of choroidal neovascularization related to chorioretinal folds.14
CONCLUSION
These cases serve as an addition to the growing body of literature pertaining to chorioretinal folds and their etiologies as well as a review of appropriate diagnostic conventions. Additional literature is needed with regard to epidemiology and etiology of chorioretinal folds in the general population. No identifiable health information was included in this case report.
ACKNOWLEDGMENTS
The authors thank Huey-Fen Song, OD, FAAO, for her contribution to the clinical care of case 3.
DISCLAIMER
The contents of this work do not represent the view of the Department of Veterans Affairs or the United States Government.
DISCLOSURES
None.