INTRODUCTION
Diabetes mellitus is a growing public health concern worldwide. It is estimated that 400 million people currently live with diabetes, which is projected to increase to almost 600 million by 2035.1,2 Diabetic retinopathy (DR), a microvascular occlusive disease, is the leading cause of blindness among the working-age population.2 Among diabetic individuals, the estimated prevalence of DR and proliferative DR (PDR) is 35.4% and 7.5%, respectively, with higher prevalence in type 1 diabetics.1 Historically, intervention in DR was reserved for patients at high risk of vision loss, including patients with PDR with high-risk characteristics or patients with center-involving diabetic macular edema (CI-DME). Patients with nonproliferative disease without macular edema have historically been managed with close observation, lifestyle modifications, and strict control of blood glucose levels and systemic vascular disease. Recent investigations into early intervention with anti- vascular endothelial growth factor (VEGF) in patients with severe nonproliferative DR (NPDR) without macular edema have raised the question of whether early intervention may be warranted to prevent long-term progression of disease and potentially reduce the risk of vision-threatening complications.3,4 No identifiable health information was included in this case report.
CASE INFORMATION
Case history
-
White male, age 47 years
-
Referred for diabetic eye examination by a fellow optometrist
-
No significant complaints aside from decreased near vision corrected with reading glasses
-
Type 2 diabetes for 10 years, with most recent A1C of 9.7% 2 months prior. Does not check blood sugar at home. Managed with weekly Trulicity injections.
-
Additional history of hypertension and hyperlipidemia
Other pertinent examination findings
-
Distance visual acuity 20/20 right eye, left eye
-
Normal anterior segment evaluation with no neovascularization of the iris of each eye
-
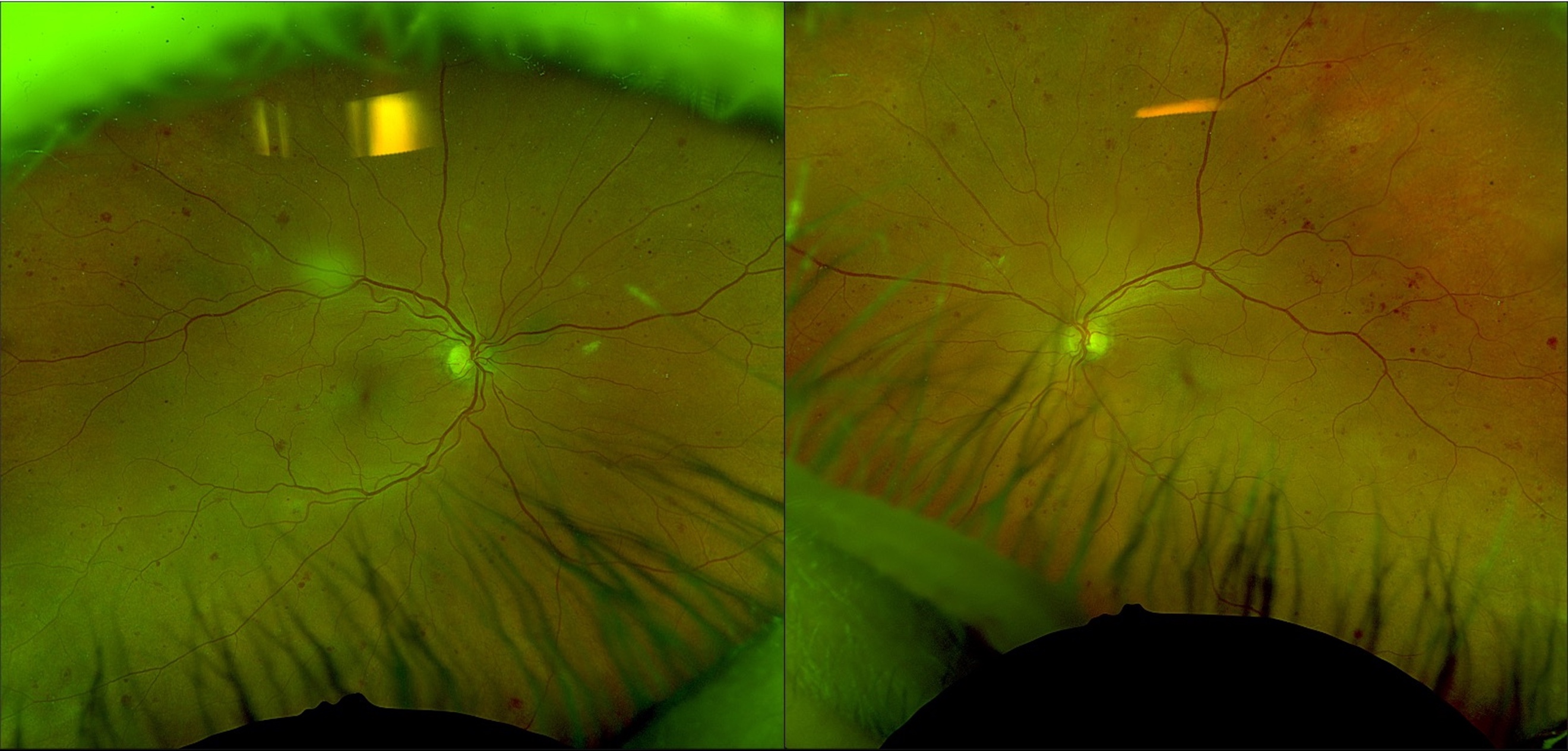
Presence of significant retinal hemorrhaging in all 4 quadrants of each eye. Presence of intraretinal microvascular abnormalities along the superior temporal arcade of the left eye (Figure 1).
-
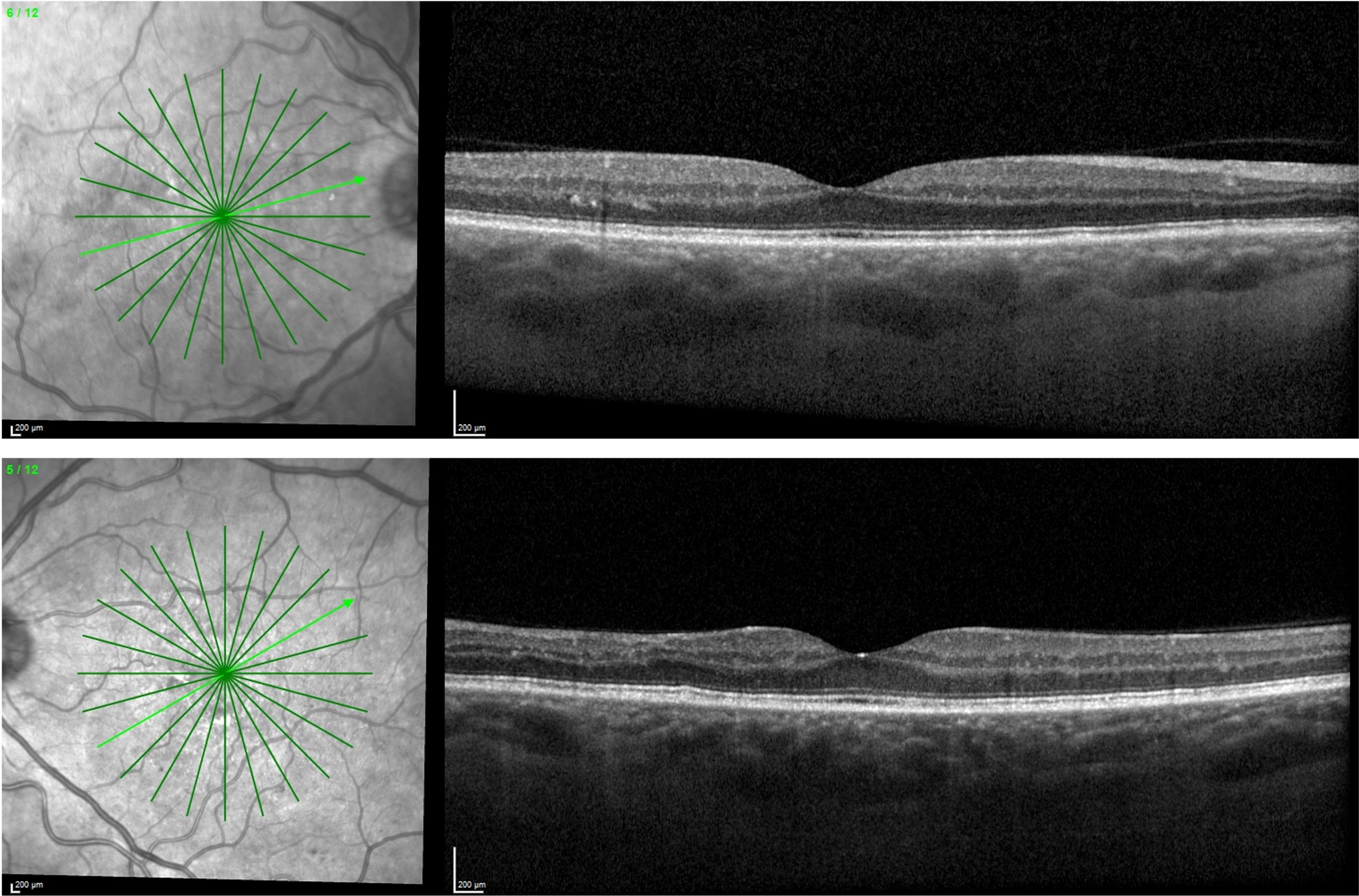
Absence of CI-DME on optical coherence tomography (Figure 2).


Diagnosis
- Severe NPDR without macular edema in each eye
POINT: Treatment of Severe NPDR with Anti-VEGF
By Jessica Haynes, OD, FAAO
A patient such as this must be educated about the importance of maintaining good blood sugar control, as well as managing concomitant vascular disease, including hypertension and hyperlipidemia. Education is required to understand that although the patient is currently asymptomatic and has good visual acuity, significant damage has already occurred to the retinal vasculature, and the patient is at risk for vision loss due to complications such as macular edema and development of PDR. Although a patient with severe NPDR without macular edema could be monitored closely at 3 to 4 month intervals without intervention, in a highly motivated and educated patient, initiation of anti-VEGF injections has been shown to reduce their level of DR and decrease the occurrence of sight-threatening complications, including CI-DME.3,4
The PANORMA study, a 100-week randomized clinical trial, compared the outcomes of moderately severe to severe NPDR without macular edema treated with intravitreal aflibercept vs sham injections.3 A total of 402 individuals were randomly assigned into 3 cohorts. A total of 135 eyes received intravitreal aflibercept 2 mg every 16 weeks after 3 loading monthly injections and one 8-week interval. A total of 134 eyes received intravitreal aflibercept 2 mg every 8 weeks after 5 loading monthly injections followed by as needed (PRN) treatment between year 1 and 2 based on DR severity score (DRSS). A total of 133 eyes received sham injections, receiving treatment only if sight-threatening complications arose.
The major outcome measures included a 2-step improvement in DRSS, occurrence of vision-threatening complications (including complications of PDR and iris neovascularization), and occurrence of CI-DME. After 100 weeks, the authors concluded that receiving intravitreal aflibercept 2mg significantly improved DRSS. At 100 weeks, 62.2% of patients treated every 16 weeks had a 2-step reduction in their DRSS, as did 50% in the every-8-weeks/PRN group. This was compared with only 12.8% of patients receiving sham.
In addition, treatment with aflibercept significantly reduced vision-threatening complications and the development of CI-DME compared with those receiving sham injections. At 100 weeks, 50.4% of eyes in the sham group developed vision-threatening complications and/or CI-DME vs only 16.3% in the every-16-weeks treatment group and 18.7% in the every-8-weeks/PRN treatment group.
With these striking results, a patient such as the one above can be educated that by receiving intravitreal injections every 16 weeks (about every 4 months following a loading dose), we have a 60% chance to significantly reduce his or her level of DR, and we can take the chance of developing sight-threatening complications from 50% down to only about 16%. It is important to note that compliance with treatment is extremely important and that although risk of sight-threatening complications is much lessened, it is not totally eliminated. Thus, there is still importance of close follow-up and adjustment of treatment if needed.
COUNTERPOINT: Monitor Without Treatment
By Rachel Steele, OD
Although this patient remains a good candidate for treatment with anti-VEGF per the outcomes of the PANORAMA trial, controversy exists over whether earlier initiation of anti-VEGF truly translates into long-term improvement in visual outcomes. The main outcome of 2-step reduction in DRSS in the PANORAMA trial has been criticized as improving a clinical picture but not ultimate visual outcomes. In addition, requirement for long-term compliance, greater treatment burden, risk of side effects from injections, and loss of benefit with discontinuation of treatment are all downsides for use of anti-VEGF in those with severe NPDR.
In post hoc analyses of PANORAMA, of the eyes that developed vision-threatening complications, a greater percentage of eyes randomized to the control group went on to lose 5 Early Treatment Diabetic Retinopathy Study (ETDRS) letters compared with those randomized to aflibercept; however, the authors noted that discontinuation of aflibercept injections or less frequent injections “may lead to PDR-related complications,”3 and suggested that regular treatment intervals were necessary to maintain DRSS improvement and decrease the risk of vision-threatening complications. Ultimately, there was no significant difference in visual acuity between eyes that were treated with aflibercept vs sham injections after 2 years. However, this requires careful monitoring and initiation of treatment should sight-threatening complications arise.
The Diabetic Retinopathy Clinical Research Network similarly evaluated treatment of moderate to severe NPDR without CI-DME in Protocol W.4 Eyes were randomized to receive either aflibercept 2 mg or sham injections at 1, 2, and 4 months and then every 4 weeks for 2 years. Of 399 participants, 200 eyes were randomized to receive aflibercept 2 mg and 199 eyes received sham injections. The study’s main outcome measures were development of either PDR or CI-DME. Results of the study showed that eyes randomized to aflibercept 2 mg had a significantly lower probability of developing PDR or CI-DME at 2 years. Additionally, a greater percentage of eyes receiving aflibercept 2 mg had a 2-step improvement in DRSS compared with the sham group. However, similar to PANORMA, the study concluded that regular treatment with aflibercept 2 mg did not “confer visual acuity benefit compared with observation with aflibercept 2mg initiated only after development of PDR or CI-DME.”4 The authors remarked that careful observation with treatment after development of vision-threatening complications may be sufficient to either recover vision loss or prevent vision loss.
More recently, data from the 4-year extension of Protocol W became available.5 After 4 years, the likelihood of developing PDR in the aflibercept 2 mg group was 27.9% vs 49% in the sham group. The probability of developing CI-DME was 11.3% in the aflibercept group vs 19.1% in the sham group. Similar to the 2-year Protocol W and PANORAMA studies, there was a greater improvement in DRSS in the aflibercept 2 mg group. But still, there was no significant difference in visual acuity outcomes between the 2 groups at 4 years. The authors concluded that based on the evidence gained from the study, there was no evidence to suggest that early treatment intervention in nonproliferative retinopathy without macular edema conferred any visual benefit out to 4 years when compared with close observation and treatment when vision-threatening complications arose. Although early treatment did reduce the risk of development of PDR and CI-DME, it did not eliminate the likelihood of progression.5
Although early intravitreal anti-VEGF was shown to decrease the risk of future vision-threatening complications, treatment needs to be maintained at regular intervals to remain beneficial, which may add to the overall treatment burden for patients. Although both PANORAMA and Protocol W demonstrated that early anti-VEGF improves DRSS, there is debate over whether improvement in DRSS truly represents improvement in overall disease.3,5–7 Recent studies by Couturier et al and Bonnin et al demonstrated that intravitreal anti-VEGF, though stabilizing the permeability of retinal microvasculature, does not result in reperfusion of ischemic capillary beds. DR lesions such as microaneurysms or intraretinal hemorrhages, though a sign of ongoing microvascular disease, do not present the greatest risk for progression to PDR. Ischemia and capillary nonperfusion drive progression to proliferative disease. Despite improvements in DRSS, which accounts for the number of DR lesions, these patients are still at risk of proliferative disease because areas of nonperfusion remain despite treatment.
Because of the long-term results of Protocol W, a patient such as this can be educated that although earlier intervention is an option, there is ultimately no evidence of altered long-term visual outcomes. Although treatment can be deferred for this patient at the time being, success still critically hinges on close observation and prompt initiation of treatment should sight-threatening complications arise. This must be heavily emphasized to the patient alongside the importance of improved blood sugar control and control of concomitant vascular disease.
Should Laser Be Considered for Severe NPDR?
Pan-retinal photocoagulation (PRP) is regarded as the standard of care for individuals with PDR.8 PRP is thought to control retinal or anterior segment neovascularization by destroying metabolically active retinal tissue, which decreases the overall oxygen demand from the tissue by reducing proangiogenic factors.8,9 PRP has long been reserved for patients with proliferative disease to reduce the long-term risk of vision loss from complications of proliferative disease rather than improve vision.
The Diabetic Retinopathy Study (DRS) and ETDRS investigated the use of PRP in nonproliferative retinopathy. In the DRS, patients had one eye receive PRP and one eye as control. At 2 years, the overall risk of severe vision loss was 3.2% in the control eyes vs 2.8% in the eyes with PRP.9 Although they found that a greater portion of the eyes without PRP went on to develop proliferative disease within the year, they did not recommend PRP for all patients with NPDR. Because of the risk of severe vision loss being low between the treated and untreated severe NPDR groups, and because of the side effects of PRP treatment such as loss of peripheral vision, the investigators recommended reserving PRP for eyes with PDR with high-risk characteristics.
In the ETDRS, patients with severe NPDR had one eye receive PRP and the other eye defer PRP. The eyes with deferred PRP had significantly higher rates of conversion to PDR at 1, 3, and 5 years; however, at 5 years, the comparison of severe vision loss between the early and deferred PRP groups was 2.6% and 3.7%, respectively.10 Although the risk of severe vision loss was similar between the groups, the ETDRS group did suggest that prophylactic PRP could be considered in select individuals with severe NPDR.
PRP leads to destruction of retinal tissue that can translate into loss of peripheral vision and reduction in night vision. Even in PDR, the use of heavy PRP has lessened significantly because of the ability to supplement with anti-VEGF. Although the utilization of PRP in those with severe NPDR is significantly less than in those with PDR, some physicians may still use the tactic in select patient populations with severe NPDR, such as those who cannot maintain compliance with follow-up or those who have had poor outcomes from PDR in the fellow eye or found it difficult to control PDR in the fellow eye.
With our current patient, PPR was not recommended by either provider.
CONCLUSIONS
Translating the results of these trials to everyday practice presents significant challenges for the practitioner, given that many patients do not understand the significant risk of future worsening in their vision or the necessity of frequent careful observation. In every treatment decision, there must be an individualized discussion with the patient about the risk presented by their disease and the potential risks and benefits conferred by any treatment intervention. Although PANORAMA and Protocol W demonstrated that early treatment with anti-VEGF reduced the rates of disease progression, they did not demonstrate that there was any visual benefit conferred by early treatment, at least up to 4 years.
Considerations for treatment initiation with anti-VEGF in those with severe NPDR without macular edema include patient preferences, blood sugar control, systemic comorbidities, ability to comply with treatment, ability to comply with follow-ups, financial obligations, and side effects of treatment. Although earlier treatment initiation is an option, given the lack of long-term improvement in visual acuity outcomes, practitioners may also continue managing these patients with frequent careful observation.
DISCLOSURES
Dr Haynes is a paid speaker for Heidelberg Engineering and Zeiss. She is a consultant for Regeneron. Dr Steele has no financial disclosures.